

Immune variations throughout the course of tuberculosis treatment and its relationship with adrenal hormone changes in HIV-1 patients co-infected with Mycobacterium tuberculosis
- PMID: 33434785
- PMCID: PMC7965356
- DOI: 10.1016/j.tube.2020.102045
Immune variations throughout the course of tuberculosis treatment and its relationship with adrenal hormone changes in HIV-1 patients co-infected with Mycobacterium tuberculosis
Abstract
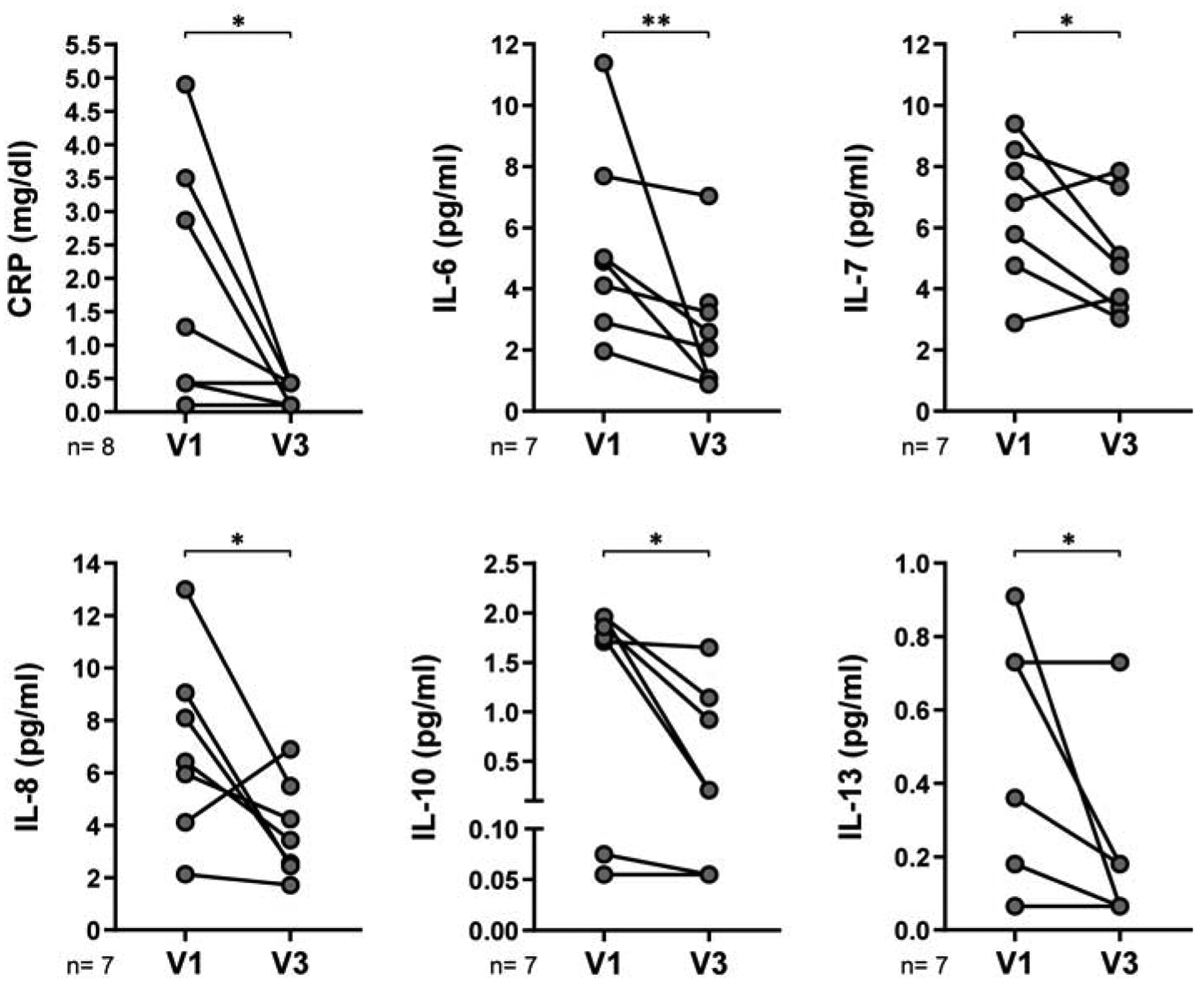
HIV infection is a major risk factor predisposing for Mycobacterium tuberculosis infection and progression to active tuberculosis (TB). As host immune response defines the course of infection, we aimed to identify immuno-endocrine changes over six-months of anti-TB chemotherapy in HIV+ people. Plasma levels of cortisol, DHEA and DHEA-S, percentages of CD4+ regulatory T cell subsets and number of IFN-γ-secreting cells were determined. Several cytokines, chemokines and C-reactive protein levels were measured. Results were correlated with clinical parameters as predictors of infection resolution and compared to similar data from HIV+ individuals, HIV-infected persons with latent TB infection and healthy donors. Throughout the course of anti-TB/HIV treatment, DHEA and DHEA-S plasma levels raised while cortisol diminished, which correlated to predictive factors of infection resolution. Furthermore, the balance between cortisol and DHEA, together with clinical assessment, may be considered as an indicator of clinical outcome after anti-TB treatment in HIV+ individuals. Clinical improvement was associated with reduced frequency of unconventional Tregs, increment in IFN-γ-secreting cells, diminution of systemic inflammation and changes of circulating cytokines and chemokines. This study suggests that the combined anti-HIV/TB therapies result in partial restoration of both, immune function and adrenal hormone plasma levels.
Keywords: Adrenal hormones; Cytokines; HIV-TB coinfection; Prospective study; Regulatory T cells; Tuberculosis.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest
The authors declare that they have no competing interests.
Figures






Similar articles
-
Dynamics of adrenal steroids are related to variations in Th1 and Treg populations during Mycobacterium tuberculosis infection in HIV positive persons.PLoS One. 2012;7(3):e33061. doi: 10.1371/journal.pone.0033061. Epub 2012 Mar 14. PLoS One. 2012. PMID: 22431997 Free PMC article.
-
HIV-TB coinfection impairs CD8(+) T-cell differentiation and function while dehydroepiandrosterone improves cytotoxic antitubercular immune responses.Eur J Immunol. 2015 Sep;45(9):2529-41. doi: 10.1002/eji.201545545. Epub 2015 Jun 22. Eur J Immunol. 2015. PMID: 26047476
-
7-oxo-DHEA enhances impaired M. tuberculosis-specific T cell responses during HIV-TB coinfection.J Biomed Sci. 2020 Jan 6;27(1):20. doi: 10.1186/s12929-019-0604-z. J Biomed Sci. 2020. PMID: 31906962 Free PMC article.
-
The Immune Response to Mycobacterium tuberculosis in HIV-1-Coinfected Persons.Annu Rev Immunol. 2018 Apr 26;36:603-638. doi: 10.1146/annurev-immunol-042617-053420. Epub 2018 Feb 28. Annu Rev Immunol. 2018. PMID: 29490165 Review.
-
State-of-the-Art Review of HIV-TB Coinfection in Special Populations.Clin Pharmacol Ther. 2018 Dec;104(6):1098-1109. doi: 10.1002/cpt.1221. Epub 2018 Oct 26. Clin Pharmacol Ther. 2018. PMID: 30137652 Review.
References
-
- World Health Organization. Global tuberculosis report 2019. 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
