

Combining Sorafenib and Immunosuppression in Liver Transplant Recipients with Hepatocellular Carcinoma
- PMID: 33435321
- PMCID: PMC7826978
- DOI: 10.3390/ph14010046
Combining Sorafenib and Immunosuppression in Liver Transplant Recipients with Hepatocellular Carcinoma
Abstract
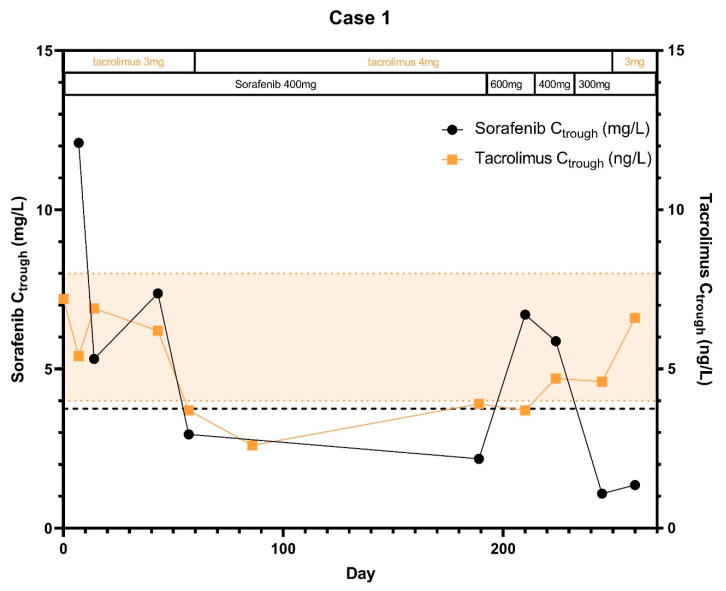
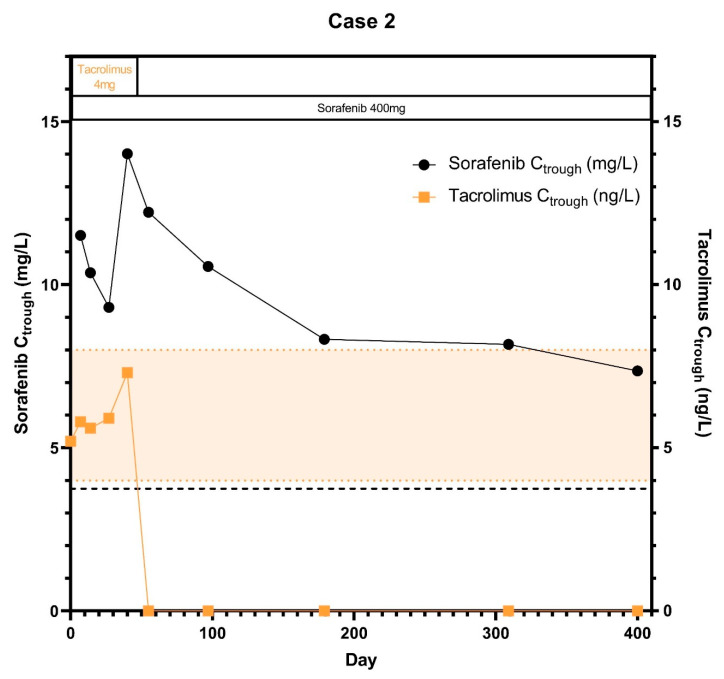
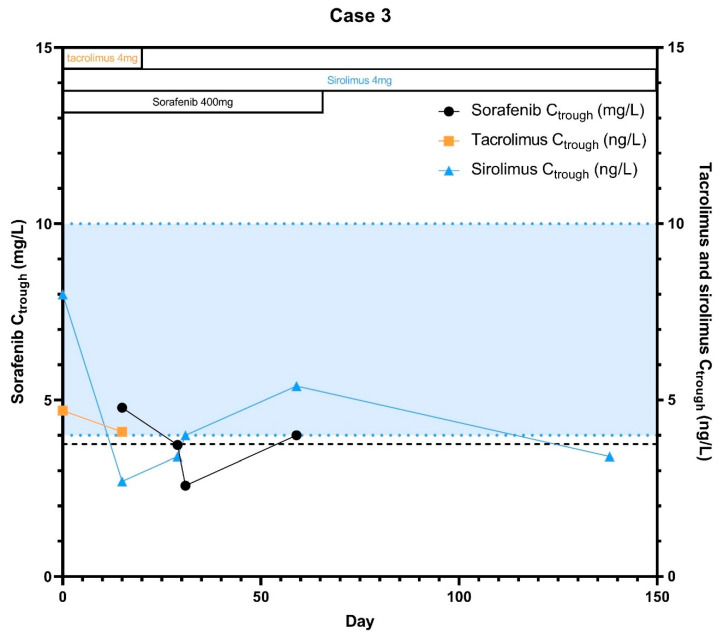
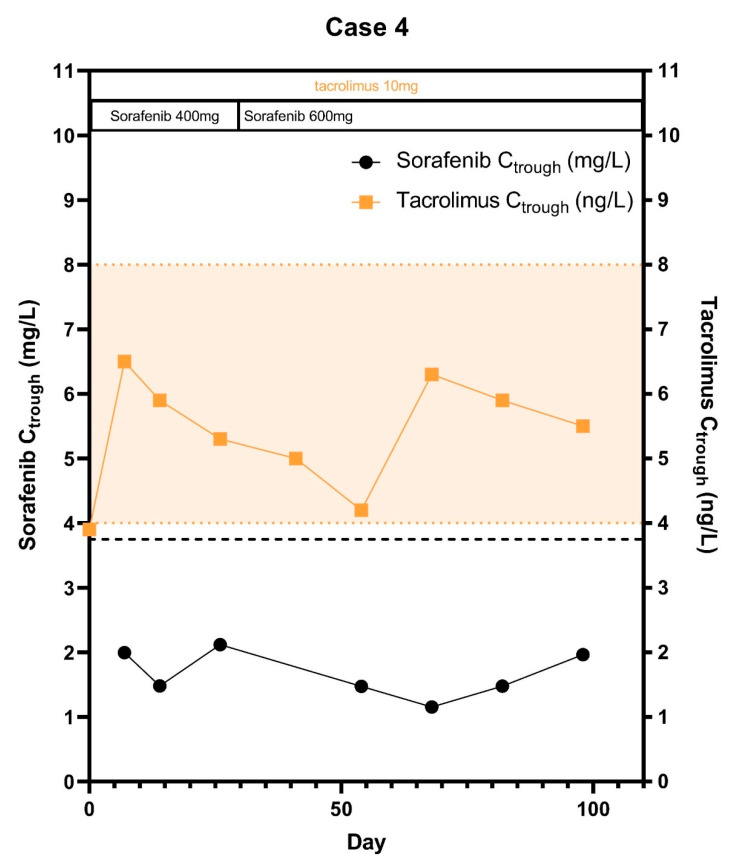
Hepatocellular carcinoma (HCC) recurrence after liver transplantation occurs in approximately 20% of patients. Most of these patients use immunosuppressant drugs. Meanwhile, patients with HCC recurrence are frequently treated with the small molecule kinase inhibitor (SMKI) sorafenib. However, sorafenib and many immunosuppressants are substrates of the same enzymatic pathways (e.g., CYP3A4), which may potentially result in altered SMKI or immunosuppressant plasma levels. Therefore, we investigated changes in drug exposure of both sorafenib and immunosuppressants over time in four patients with systemic immunosuppressant and sorafenib treatment after HCC recurrence. In this study, sorafenib exposure declined over time during combined treatment with immunosuppressants, while two patients also experienced declining tacrolimus plasma levels. Importantly, patients were unable to increase the sorafenib dose higher than 200 mg b.i.d. without experiencing significant toxicity. We recommend to treat patients using both sorafenib and immunosuppressants with a sorafenib starting dose of 200 mg b.i.d.
Keywords: HCC; liver transplantation; sorafenib.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Iavarone M., Invernizzi F., Czauderna C., Sanduzzi-Zamparelli M., Bhoori S., Amaddeo G., Manini M.A., López M.F., Anders M., Pinter M., et al. Preliminary experience on safety of regorafenib after sorafenib failure in recurrent hepatocellular carcinoma after liver transplantation. Am. J. Transplant. 2019;19:3176–3184. doi: 10.1111/ajt.15551. - DOI - PubMed
-
- Zimmerman M.A., Ghobrial R.M., Tong M.J., Hiatt J.R., Cameron A.M., Hong J., Busuttil R.W. Recurrence of Hepatocellular Carcinoma Following Liver Transplantation: A Review of Preoperative and Postoperative Prognostic Indicators. Arch. Surg. 2008;143:182–188. doi: 10.1001/archsurg.2007.39. - DOI - PubMed
-
- Sposito C., Mariani L., Germini A., Reyes M.F., Bongini M., Grossi G., Bhoori S., Mazzaferro V. Comparative efficacy of sorafenib versus best supportive care in recurrent hepatocellular carcinoma after liver transplantation: A case-control study. J. Hepatol. 2013;59:59–66. doi: 10.1016/j.jhep.2013.02.026. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
