

A Rare Entity-Percutaneous Lead Extraction in a Very Late Onset Pacemaker Endocarditis: Case Report and Review of Literature
- PMID: 33435384
- PMCID: PMC7827933
- DOI: 10.3390/diagnostics11010096
A Rare Entity-Percutaneous Lead Extraction in a Very Late Onset Pacemaker Endocarditis: Case Report and Review of Literature
Abstract
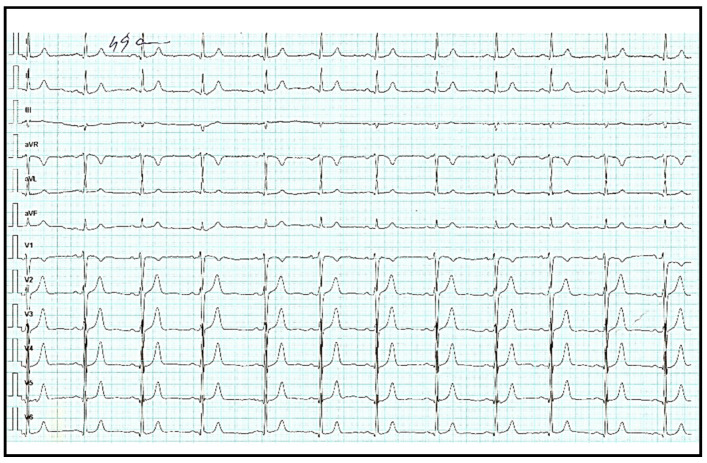
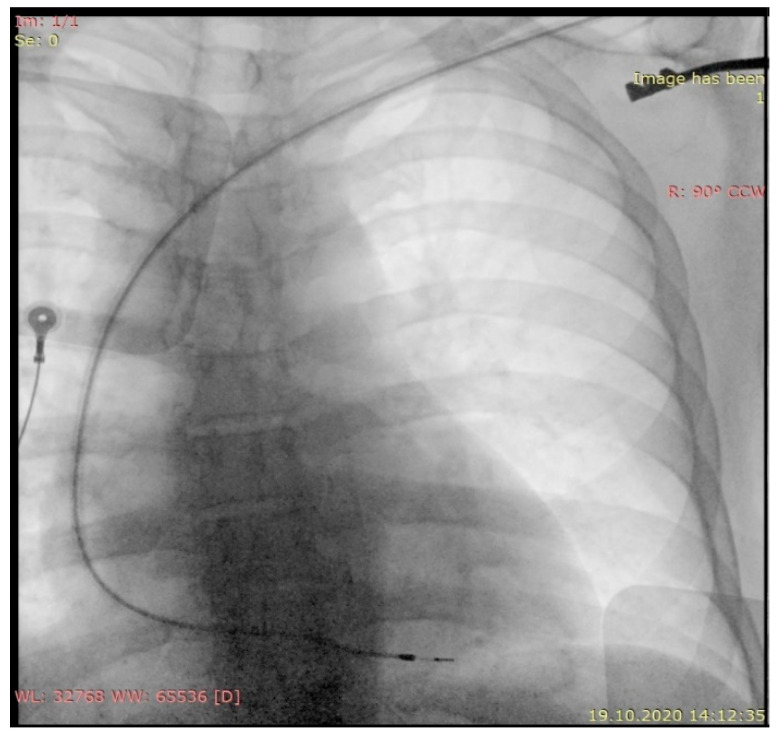
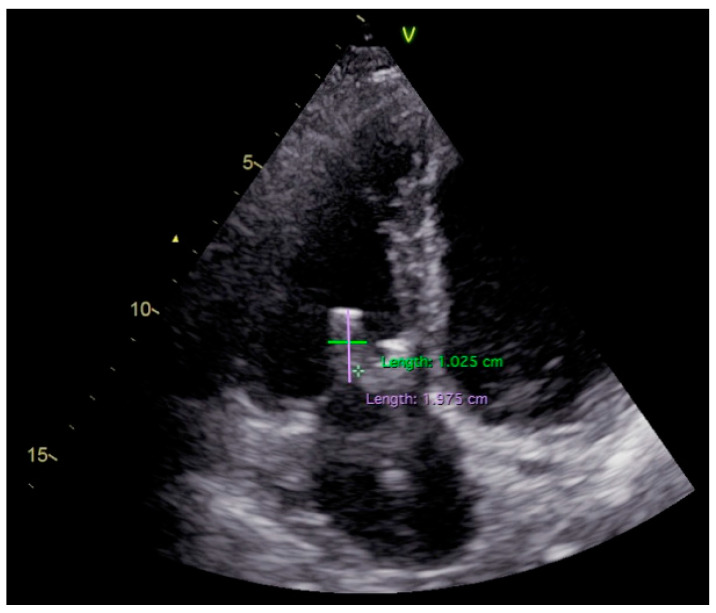
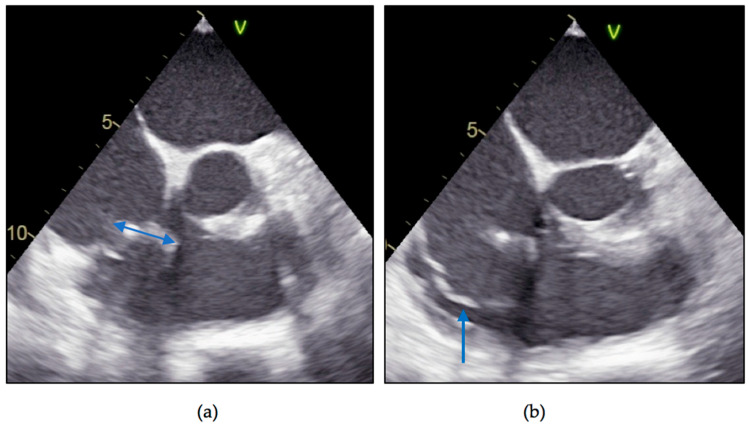
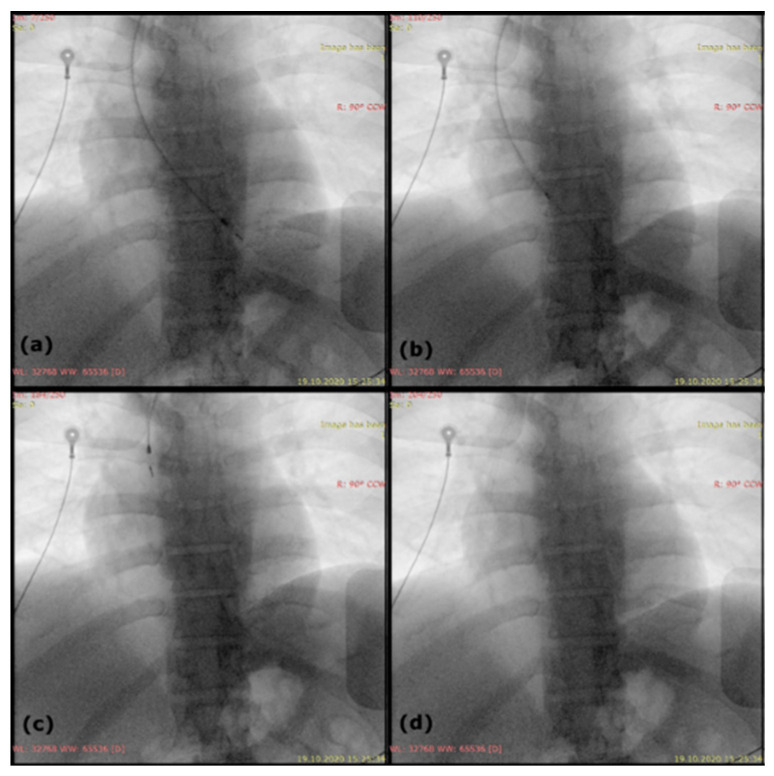
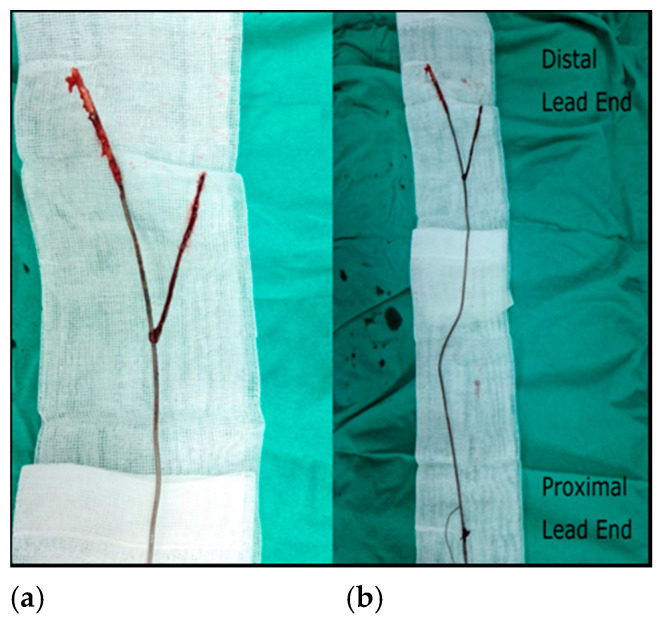
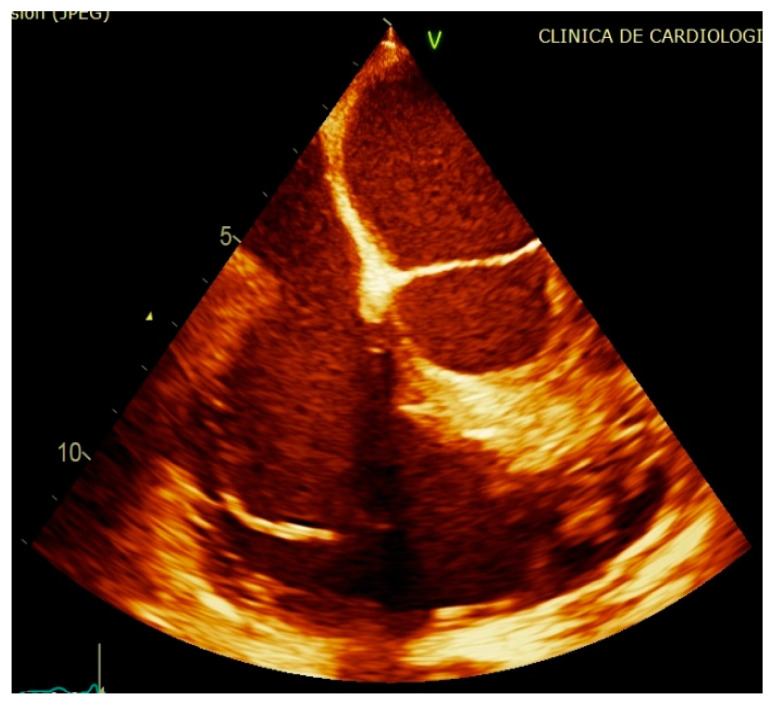
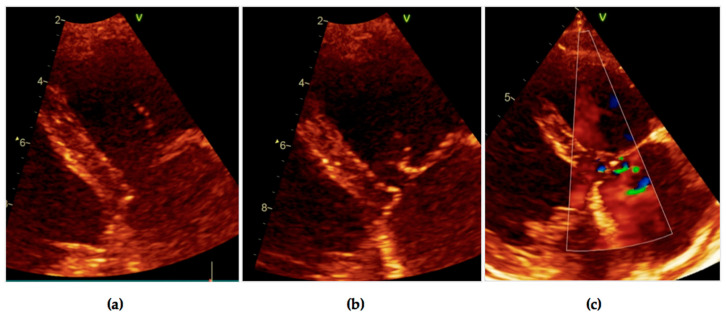
The number of infections related to cardiac implantable electronic devices (CIEDs) has increased as the number of devices implanted around the world has grown exponentially in recent years. CIED complications can sometimes be difficult to diagnose and manage, as in the case of lead-related infective endocarditis. We present the case of a 48-year-old male diagnosed with Staphylococcus aureus device-related infective endocarditis, 12 years after the implant of a single chamber pacemaker. A recent history of the patient includes two urinary catheterizations due to obstructive uropathy in the context of a prostatic adenoma, 2 months previously, both without antibiotic prophylaxis; no other possible entry sites were found and no history of other invasive procedures. After initiation of antibiotic therapy according to antibiotic susceptibility testing, we decided to remove the right ventricular passive fixation lead along with the vegetation and pacemaker generator; because of severe lead adhesions in the costoclavicular region, and especially in the right ventricle, we needed mechanical sheaths to remove the abundant fibrous tissue that encompassed the lead. After a difficult, but successful, lead extraction along with a large vegetation and 6 weeks' antibiotic therapy, the clinical and biological evolution was favorable, without reappearance of symptoms. While very late lead endocarditis is a rarity, late lead-related infective endocarditis (more than 12 months elapsed since implant) is not an exception; this is why we find that endocarditis prophylaxis should be reconsidered in certain patient categories, our patient being proof that procedures with neglectable endocarditis risk according to the guidelines can lead to bacterial endocarditis.
Keywords: cardiac device; endocarditis; infection; late lead extraction; late lead-related infective endocarditis; pacemaker lead endocarditis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Intractable late onset pacemaker endocarditis and complications case report.Heliyon. 2024 Nov 1;10(21):e40073. doi: 10.1016/j.heliyon.2024.e40073. eCollection 2024 Nov 15. Heliyon. 2024. PMID: 39553610 Free PMC article.
-
Prognosis after lead extraction in patients with cardiac implantable electronic devices infection: Comparison of lead-related infective endocarditis with pocket infection in a Japanese single-center experience.J Arrhythm. 2019 Jun 28;35(4):654-663. doi: 10.1002/joa3.12164. eCollection 2019 Aug. J Arrhythm. 2019. PMID: 31410236 Free PMC article.
-
A rare case of pacemaker lead endocarditis successfully treated with open heart surgery.J Infect Dev Ctries. 2019 Nov 30;13(11):1068-1071. doi: 10.3855/jidc.11941. J Infect Dev Ctries. 2019. PMID: 32087081
-
Candida and cardiovascular implantable electronic devices: a case of lead and native aortic valve endocarditis and literature review.Mycoses. 2015 Nov;58(11):637-41. doi: 10.1111/myc.12391. Epub 2015 Sep 25. Mycoses. 2015. PMID: 26403965 Review.
-
[Infective endocarditis on probe of pacemaker].Tunis Med. 2009 Sep;87(9):610-5. Tunis Med. 2009. PMID: 20180384 Review. French.
Cited by
-
Early, Delayed and Late Cardiac Implantable Electronic Device Infections: Do the Timing of Onset and Pathogens Matter?J Clin Med. 2022 Jul 6;11(14):3929. doi: 10.3390/jcm11143929. J Clin Med. 2022. PMID: 35887692 Free PMC article.
-
A pacemaker lead infection as a complication of a discitis post fall in an elderly: A case report.J Family Med Prim Care. 2023 Jun;12(6):1234-1236. doi: 10.4103/jfmpc.jfmpc_207_23. Epub 2023 Jun 30. J Family Med Prim Care. 2023. PMID: 37636195 Free PMC article.
-
Reduced fibrous capsule elastic fibers from biologic ECM-enveloped CIEDs in minipigs, supported with a novel compression mechanics model.Biomed Mater Eng. 2023;34(4):289-304. doi: 10.3233/BME-221488. Biomed Mater Eng. 2023. PMID: 36617774 Free PMC article.
References
-
- Rossi M., Musolino G., Serraino G.F., Renzulli A. Device-Related Endocarditis and Infected Leads Extraction: The Dark Side of The Moon. In: Attila R., editor. Current Issues and Recent Advances in Pacemaker Therapy. IntechOpen Limited; London, UK: 2012. pp. 159–163.
-
- Vilacosta I., Olmos C., De Agustin A., Lopez J., Islas F., Sarriá C., Ferrera C., Ferrera C., Sánchez-Enrique C., Vivas D., et al. The diagnostic ability of echocardiography for infective endocarditis and its associated complications. Expert Rev. Cardiovasc. Ther. 2015;13:1225–1236. doi: 10.1586/14779072.2015.1096780. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
