

Preliminary report of modified expansive laminoplasty in the treatment of thoracic ossification of the ligamentum flavum
- PMID: 33435762
- PMCID: PMC7809308
- DOI: 10.1177/0300060520985383
Preliminary report of modified expansive laminoplasty in the treatment of thoracic ossification of the ligamentum flavum
Abstract
Objective: This study was performed to evaluate the role of posterior suspension of the laminae-ossification of the ligamentum flavum complex combined with miniplate fixation (modified expansive thoracic laminoplasty) in treating thoracic ossification of the ligamentum flavum (TOLF).
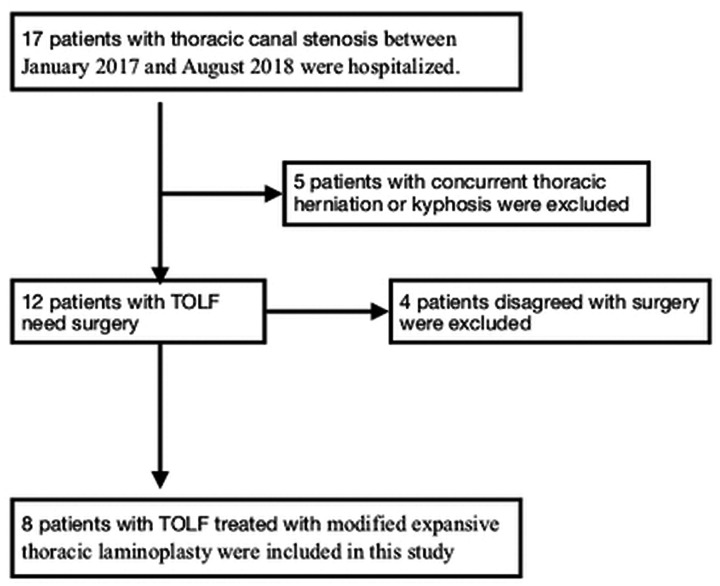
Methods: Eight patients with TOLF treated by modified expansive thoracic laminoplasty were retrospectively analyzed. Their general information, operative time, intraoperative blood loss, and postoperative complications were recorded. Neurological functional recovery was evaluated by the modified Japanese Orthopaedic Association (mJOA) score and Hirabayashi recovery rate preoperatively, postoperatively, and at the final follow-up. Preoperative and postoperative imaging was performed, and the decompression range and internal fixation positioning were evaluated.
Results: The mJOA score significantly improved from 4.63 points preoperatively to 9.0 points at the final follow-up (Hirabayashi recovery rate of 77.75%). Postoperative computed tomography and magnetic resonance imaging revealed sufficient decompression of the surgical segment. At the final follow-up, the internal implants were well-placed, the lamina-ligamentum flavum complex showed no significant displacement, and neurological functional recovery was satisfactory.
Conclusion: Surgical treatment of TOLF is complicated and high-risk. Characterized by simplicity and sufficient decompression, modified expansive thoracic laminoplasty can reduce the risk of cerebrospinal fluid leakage and nerve injury with satisfactory neurological functional recovery.
Keywords: Thoracic ossification of the ligamentum flavum; decompression; diagnostic imaging; expansive laminoplasty; neurological functional recovery; spinal cord compression.
Conflict of interest statement
Figures


References
-
- Sun X, Sun C, Liu X, et al. The frequency and treatment of dural tears and cerebrospinal fluid leakage in 266 patients with thoracic myelopathy caused by ossification of the ligamentum flavum. Spine (Phila Pa 1976) 2012; 37: E702–E707. doi: 10.1097/BRS.0b013e31824586a8. - PubMed
-
- Sun J, Sun K, Shi J, et al. The bridge crane technique for the treatment of the severe thoracic ossification of the ligamentum flavum with myelopathy. Eur Spine J 2018; 27: 1846–1855. doi: 10.1007/s00586-018-5683-0. - PubMed
-
- Kang KC, Lee CS, Shin SK, et al. Ossification of the ligamentum flavum of the thoracic spine in the Korean population. J Neurosurg Spine 2011; 14: 513–519. doi: 10.3171/2010.11.SPINE10405. - PubMed
-
- Liao CC, Chen TY, Jung SM, et al. Surgical experience with symptomatic thoracic ossification of the ligamentum flavum. J Neurosurg Spine 2005; 2: 34–39. doi: 10.3171/spi.2005.2.1.0034. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
