

Testing, infection and complication rates of COVID-19 among people with a recent history of homelessness in Ontario, Canada: a retrospective cohort study
- PMID: 33436450
- PMCID: PMC7843074
- DOI: 10.9778/cmajo.20200287
Testing, infection and complication rates of COVID-19 among people with a recent history of homelessness in Ontario, Canada: a retrospective cohort study
Abstract
Background: People with a recent history of homelessness are believed to be at high risk of infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and, when infected, complications of coronavirus disease 2019 (COVID-19). We describe and compare testing for SARS-CoV-2, test positivity and hospital admission, receipt of intensive care and mortality rates related to COVID-19 for people with a recent history of homelessness versus community-dwelling people as of July 31, 2020.
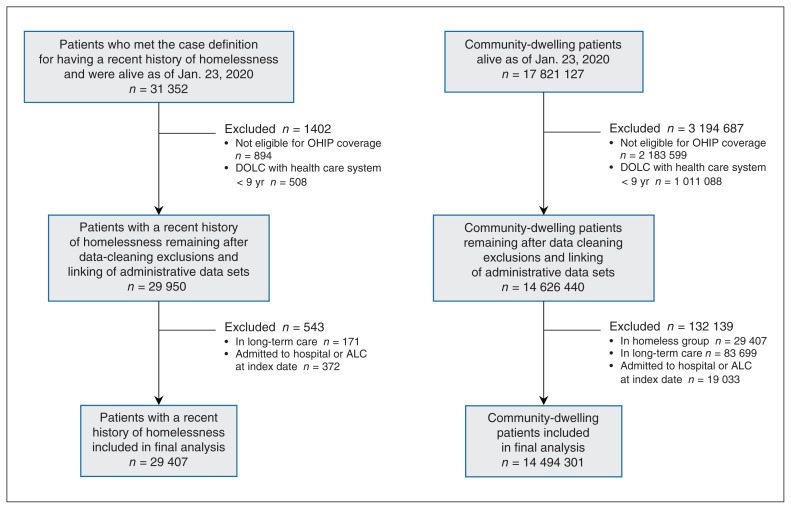
Methods: We conducted a population-based retrospective cohort study in Ontario, Canada, between Jan. 23 and July 31, 2020, using linked health administrative data among people who either had a recent history of homelessness or were dwelling in the community. People were included if they were eligible for provincial health care coverage and not living in an institutionalized facility on Jan. 23, 2020. We examined testing for SARS-CoV-2, test positivity and complication outcomes of COVID-19 (hospital admission, admission to intensive care and death) within 21 days of a positive test result. Extended multivariable Cox proportional hazard models were used to estimate adjusted hazard ratios (HRs) in 3 time periods: preshutdown (Jan. 23-Mar. 13), peak (Mar. 14-June 16) and reopening (June 17-July 31).
Results: People with a recent history of homelessness (n = 29 407) were more likely to be tested for SARS-CoV-2 in all 3 periods compared with community-dwelling people (n = 14 494 301) (preshutdown adjusted HR 1.61, 95% confidence interval [CI] 1.22-2.11; peak adjusted HR 2.95, 95% CI 2.88-3.03; reopening adjusted HR 1.45, 95% CI 1.39-1.51). They were also more likely to have a positive test result (peak adjusted HR 3.66, 95% CI 3.22-4.16; reopening adjusted HR 1.76, 95% CI 1.15-2.71). In the peak period, people with a recent history of homelessness were over 20 times more likely to be admitted to hospital for COVID-19 (adjusted HR 20.35, 95% CI 16.23-25.53), over 10 times more likely to require intensive care for COVID-19 (adjusted HR 10.20, 95% CI 5.81-17.93) and over 5 times more likely to die within 21 days of their first positive test result (adjusted HR 5.73, 95% CI 3.01-10.91).
Interpretation: In Ontario, people with a recent history of homelessness were significantly more likely to be tested for SARS-CoV-2, to have a positive test result, to be admitted to hospital for COVID-19, to receive intensive care for COVID-19 and to die of COVID-19 compared with community-dwelling people. People with a recent history of homelessness should continue to be considered particularly vulnerable to SARS-CoV-2 infection and its complications.
Copyright 2021, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Outside of the submitted work, Kristin Clemens has received a research award funded in part by AstraZeneca, she has attended Merck-sponsored conferences and she has received personal fees to deliver continuing medical education talks from Sutherland Global Services Canada ULC and the Canadian Medical and Surgical Knowledge Translation Research Group. No other competing interests were declared.
Figures
References
-
- Patton J. Coronavirus: advocates threaten legal action if Toronto doesn’t step up aide for homeless population. Global News. 2020. Apr 21, [accessed 2020 Aug. 5]. Available: https://globalnews.ca/news/6847669/coronavirus-toronto-homeless-aid/
-
- Culhane D, Treglia D, Steif K, et al. Estimated emergency and observational/quarantine capacity need for the US homeless population related to COVID-19 exposure by county; projected hospitalizations, intensive care units and mortality. Berkeley (CA): Bepress; 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous