

Left ventricular fibrosis and hypertrophy are associated with mortality in heart failure with preserved ejection fraction
- PMID: 33436786
- PMCID: PMC7804435
- DOI: 10.1038/s41598-020-79729-6
Left ventricular fibrosis and hypertrophy are associated with mortality in heart failure with preserved ejection fraction
Abstract
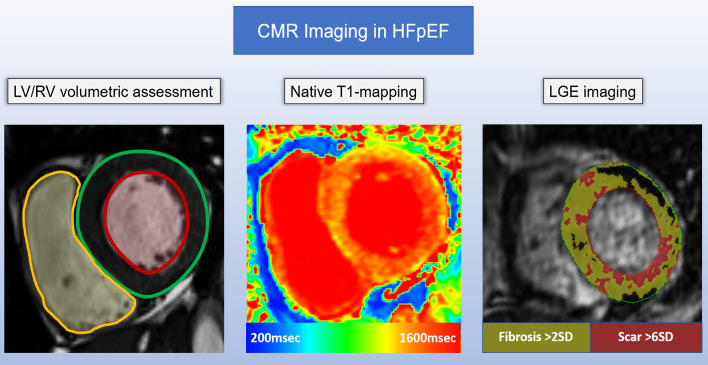
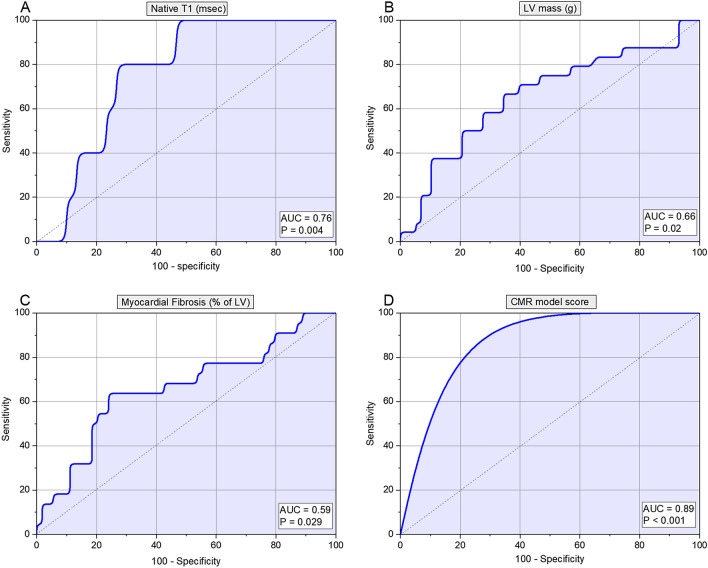
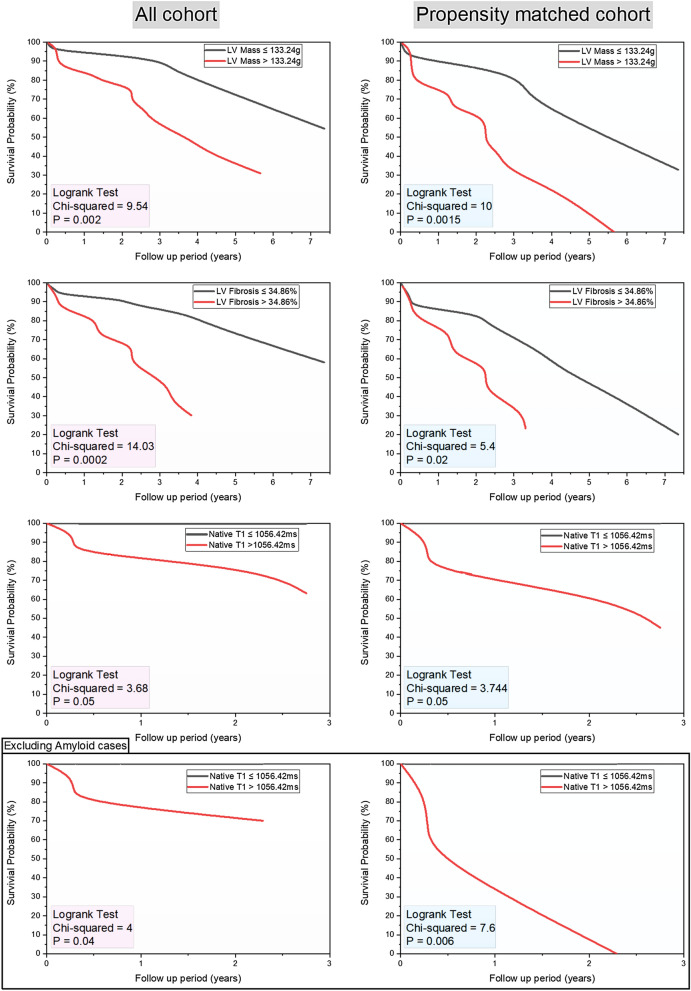
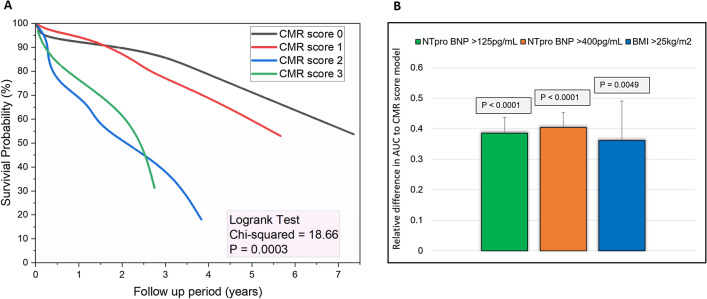
Cardiac magnetic resonance (CMR) is emerging as an important tool in the assessment of heart failure with preserved ejection fraction (HFpEF). This study sought to investigate the prognostic value of multiparametric CMR, including left and right heart volumetric assessment, native T1-mapping and LGE in HFpEF. In this retrospective study, we identified patients with HFpEF who have undergone CMR. CMR protocol included: cines, native T1-mapping and late gadolinium enhancement (LGE). The mean follow-up period was 3.2 ± 2.4 years. We identified 86 patients with HFpEF who had CMR. Of the 86 patients (85% hypertensive; 61% males; 14% cardiac amyloidosis), 27 (31%) patients died during the follow up period. From all the CMR metrics, LV mass (area under curve [AUC] 0.66, SE 0.07, 95% CI 0.54-0.76, p = 0.02), LGE fibrosis (AUC 0.59, SE 0.15, 95% CI 0.41-0.75, p = 0.03) and native T1-values (AUC 0.76, SE 0.09, 95% CI 0.58-0.88, p < 0.01) were the strongest predictors of all-cause mortality. The optimum thresholds for these were: LV mass > 133.24 g (hazard ratio [HR] 1.58, 95% CI 1.1-2.2, p < 0.01); LGE-fibrosis > 34.86% (HR 1.77, 95% CI 1.1-2.8, p = 0.01) and native T1 > 1056.42 ms (HR 2.36, 95% CI 0.9-6.4, p = 0.07). In multivariate cox regression, CMR score model comprising these three variables independently predicted mortality in HFpEF when compared to NTproBNP (HR 4 vs HR 1.65). In non-amyloid HFpEF cases, only native T1 > 1056.42 ms demonstrated higher mortality (AUC 0.833, p < 0.01). In patients with HFpEF, multiparametric CMR aids prognostication. Our results show that left ventricular fibrosis and hypertrophy quantified by CMR are associated with all-cause mortality in patients with HFpEF.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Gardin JM, et al. M-mode echocardiographic predictors of six- to seven-year incidence of coronary heart disease, stroke, congestive heart failure, and mortality in an elderly cohort (the Cardiovascular Health Study) Am. J. Cardiol. 2001;87:1051–1057. doi: 10.1016/S0002-9149(01)01460-6. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
