

Endovascular management of giant visceral artery aneurysms
- PMID: 33436829
- PMCID: PMC7803780
- DOI: 10.1038/s41598-020-80150-2
Endovascular management of giant visceral artery aneurysms
Abstract
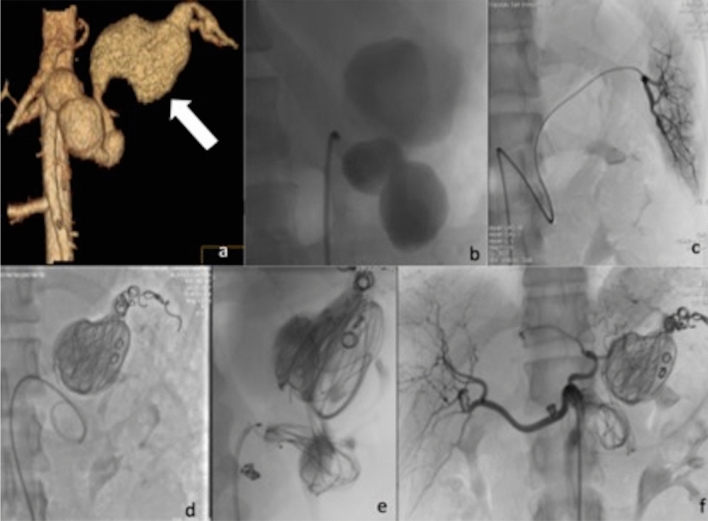
Endovascular management of small visceral artery aneurysms is an established treatment with satisfactory outcomes. However, when size exceeds 5 cm visceral aneurysms are considered as "giant" (giant visceral artery aneurysms or GVAAs) and management is significantly more complex. Between August 2007 and June 2019 eleven cases of GVAAs that were endovascularly treated were retrospectively reviewed and included in this single center study. Mean size was 80 mm (± 26.3 mm) x 46 mm (+ \-11.8 mm). Nine of the lesions were true aneurysms, and two were pseudoaneurysms. In 8 patients, the lesion was causing compression symptoms in the surrounding organs, one patient developed a contained rupture while 2 patients were completely asymptomatic. However, all patients were hemodynamically stable at the time of treatment. Technical success was defined as immediate complete exclusion of the aneurysmal sac, and clinical success as complete relief from clinical symptoms. Follow-up was performed with CT angiography, ultrasound and clinical examination. Mean follow-up was 45 months (range 6-84). Technical and clinical success were both 91%. Complications were one lack of control of contained rupture that was subsequently operated, one case of self-limiting non-target spleen embolization and one case of splenic abscess. Three patients died, one due to the contained rupture 15 days after procedure, the other two for other causes and occurred during the long-term follow-up. This series suggests that endovascular treatment of giant visceral artery aneurysms and pseudoaneuryms is a valid minimally invasive solution with very satisfactory immediate and long-term outcomes unless the aneurysm is already ruptured. A variety of endovascular tools may be required for successful treatment.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Hossian A, Reis ED, Dave SP, Kerstein MD, Hollier LH. Visceral artery aneurysms: experience in a tertiary-care center. Am. Surg. 2001;67:432–437. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
