

Hemothorax: A Review of the Literature
- PMID: 33437141
- PMCID: PMC7799890
- DOI: 10.1097/CPM.0000000000000343
Hemothorax: A Review of the Literature
Abstract
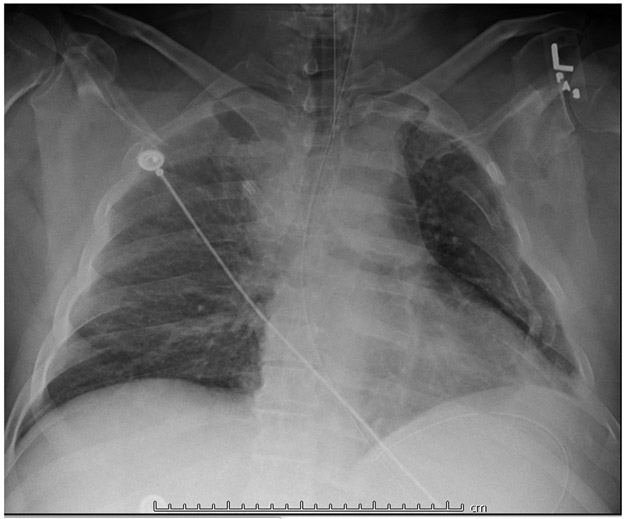
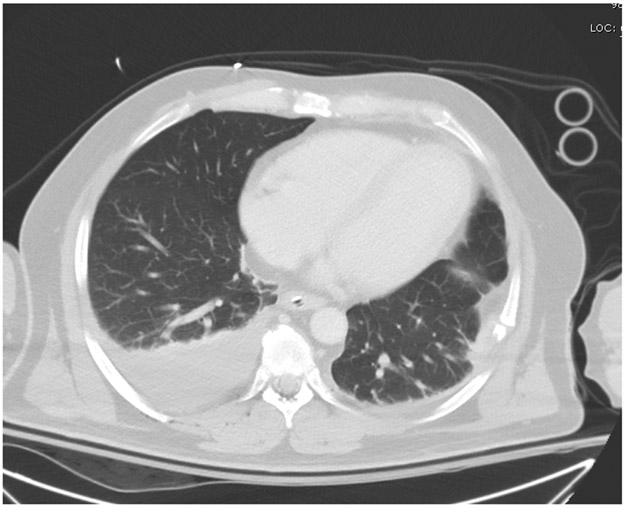
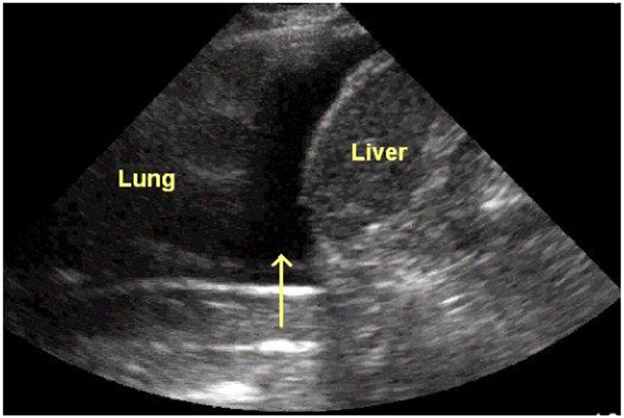
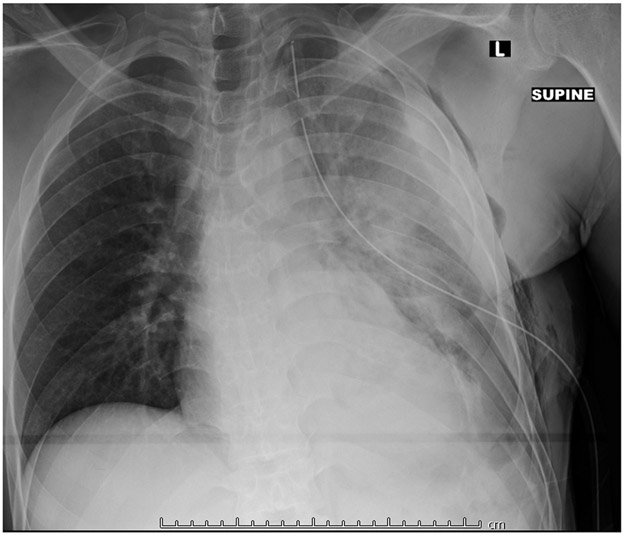
Hemothorax is a collection of blood in the pleural cavity usually from traumatic injury. Chest X-ray has historically been the imaging modality of choice upon arrival to the hospital. The sensitivity and specificity of point-of-care ultrasound, specifically through the Extended Focal Assessment with Sonography in Trauma (eFAST) protocol has been significant enough to warrant inclusion in most Level 1 trauma centers as an adjunct to radiographs.1,2 If the size or severity of a hemothorax warrants intervention, tube thoracostomy has been and still remains the treatment of choice. Most cases of hemothorax will resolve with tube thoracostomy. If residual blood remains within the pleural cavity after tube thoracostomy, it is then considered to be a retained hemothorax, with significant risks for developing late complications such as empyema and fibrothorax. Once late complications occur, morbidity and mortality increase dramatically and the only definitive treatment is surgery. In order to avoid surgery, research has been focused on removing a retained hemothorax before it progresses pathologically. The most promising therapy consists of fibrinolytics which are infused into the pleural space, disrupting the hemothorax, allowing for further drainage. While significant progress has been made, additional trials are needed to further define the dosing and pharmacokinetics of fibrinolytics in this setting. If medical therapy and early procedures fail to resolve the retained hemothorax, surgery is usually indicated. Surgery historically consisted solely of thoracotomy, but has been largely replaced in non-emergent situations by video-assisted thoracoscopy (VATS), a minimally invasive technique that shows considerable improvement in the patients' recovery and pain post-operatively. Should all prior attempts to resolve the hemothorax fail, then open thoracotomy may be indicated.
Conflict of interest statement
Conflict of Interest Statement: Steven Idell, MD, PhD serves as a Founder and Chief Scientific Officer of LTI and a member of the Board of Directors of LTI, which provided funding for preparation of the drug product and for the trial. He has an equity position (first-tier conflict of interest) in the company, as does the University of Texas Horizon Fund and the UTHSCT. He has a conflict-of-interest plan acknowledging and managing these declared conflicts of interest through the UTHSCT and the UT System. He is an inventor on a patent (USPTO 7332469) held by the UT Board of Regents and licensed to LTI. The remaining authors declare they have no such conflicts of interest.
Figures
References
-
- Bloom B, Gibbons R, Focused Assessment with Sonography for Trauma (FAST). StatPearls Publishing, 2019. at https://www.ncbi.nlm.gov/books/NBK470479/.) - PubMed
-
- O׳Keeffe M, Clark S, Khosa F, Mohammed MF, McLaughlin PD, Nicolaou S. Imaging Protocols for Trauma Patients: Trauma Series, Extended Focused Assessment With Sonography for Trauma, and Selective and Whole-body Computed Tomography. Semin Roentgenol 2016;51:130–42. - PubMed
-
- Boersma WG, Stigt JA, Smit HJ. Treatment of haemothorax. Respir Med 2010;104:1583–7. - PubMed
-
- Richardson JD, Miller FB, Carrillo EH, Spain DA. Complex thoracic injuries. Surg Clin North Am 1996;76:725–48. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources