

Preliminary results of modified interstitial MIAMI brachytherapy applicator for treatment of upper and apical vaginal tumors
- PMID: 33437304
- PMCID: PMC7787207
- DOI: 10.5114/jcb.2020.101689
Preliminary results of modified interstitial MIAMI brachytherapy applicator for treatment of upper and apical vaginal tumors
Abstract
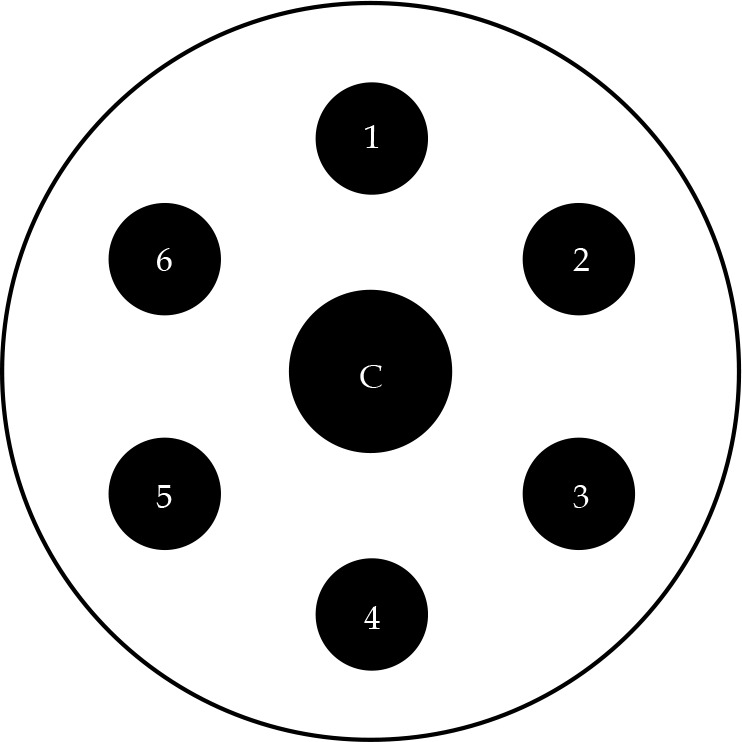
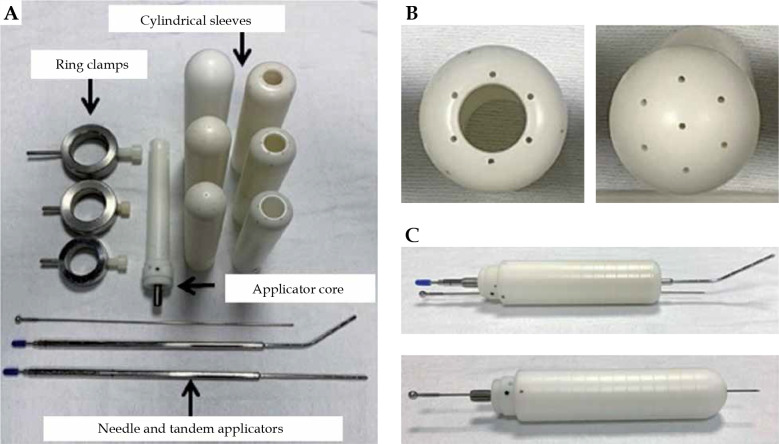
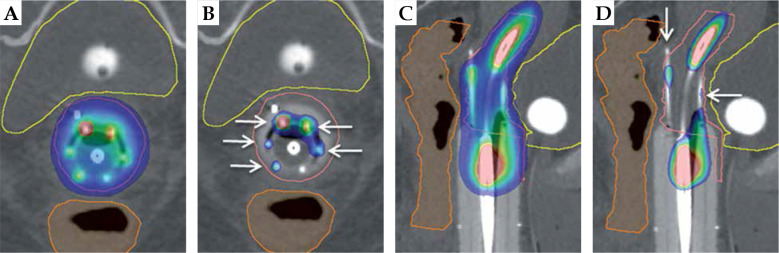
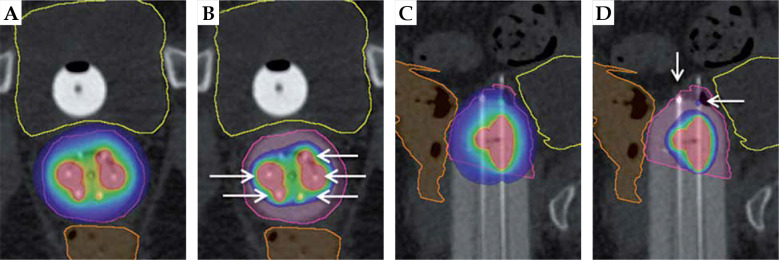
Purpose: Intracavitary vaginal brachytherapy (VBT) cylinders are limited in treating upper/apical vaginal disease due to the distance between the target and radiation source positions. Interstitial brachytherapy devices directly expose the vaginal mucosa to radiation sources, increasing morbidity. To target apical disease while limiting excessive treatment to the vaginal mucosa and organs at risk, we modified the commercially available multichannel MIAMI applicator, allowing the direct extension of needles into the apex with the protection of cylinder.
Material and methods: The device has one central plastic core with six peripheral channels. The modified device permits titanium needles to surpass the apical surface into vaginal tissue. A retrospective analysis on thirteen patients treated with this device was conducted. Patient demographics, gross tumor volume (GTV)/clinical target volume (CTV), initial diagnosis and management, toxicity data, and EQD2 data for the bladder and rectum were obtained.
Results: There were ten patients with vaginal recurrences and three with primary vaginal/cervical cancers. Mean dosage of VBT treatment was 25.5 Gy in 3-5 fractions. Mean dosage of external beam radiation therapy (EBRT) treatment was 44 Gy. Common acute toxicities included diarrhea, fatigue, cystitis, and nausea. Common chronic toxicities were pelvic pain, vaginal stenosis, and skin telangiectasia. Mean EQD2 dose for bladder and rectum were 72.3 Gy and 62.3 Gy, respectively. Ten patients had no evidence of relapse, two suffered from distant metastases, and one patient with stage IIIA cervical adenocarcinoma had loco-regional recurrence seventeen months after radiation treatment.
Conclusions: Our data suggests that the custom applicator is associated with robust dosimetric coverage, good loco-regional control, acceptable toxicity, and reduced tissue trauma. This device allows treatment of apically located vaginal tumors without significant damage to the vaginal vault and organs at risk. Additionally, it provides the flexibility to treat multiple patients with variable vaginal diameters and sizes/depths of apical tumors using a single device.
Keywords: apical tumor; endometrial cancer; multichannel; vaginal brachytherapy; vaginal cuff.
Copyright © 2020 Termedia.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Multichannel vaginal cylinder brachytherapy-Impact of tumor thickness and location on dose to organs at risk.Brachytherapy. 2015 Nov-Dec;14(6):913-8. doi: 10.1016/j.brachy.2015.08.009. Epub 2015 Sep 26. Brachytherapy. 2015. PMID: 26412618
-
Clinical applications of custom-made vaginal cylinders constructed using three-dimensional printing technology.J Contemp Brachytherapy. 2016 Jun;8(3):208-14. doi: 10.5114/jcb.2016.60679. Epub 2016 Jun 20. J Contemp Brachytherapy. 2016. PMID: 27504130 Free PMC article.
-
American Brachytherapy Society survey regarding practice patterns of postoperative irradiation for endometrial cancer: current status of vaginal brachytherapy.Int J Radiat Oncol Biol Phys. 2005 Dec 1;63(5):1502-7. doi: 10.1016/j.ijrobp.2005.04.038. Epub 2005 Aug 18. Int J Radiat Oncol Biol Phys. 2005. PMID: 16109462
-
Electronic brachytherapy for gynecological cancers - a systematic review.Rep Pract Oncol Radiother. 2023 Apr 6;28(1):79-87. doi: 10.5603/RPOR.a2023.0003. eCollection 2023. Rep Pract Oncol Radiother. 2023. PMID: 37122914 Free PMC article. Review.
-
Radiation-induced vaginal stenosis: current perspectives.Int J Womens Health. 2017 May 2;9:273-279. doi: 10.2147/IJWH.S106796. eCollection 2017. Int J Womens Health. 2017. PMID: 28496367 Free PMC article. Review.
Cited by
-
The Montreal split ring applicator: Towards highly adaptive gynecological brachytherapy using 3D-printed biocompatible patient-specific interstitial caps.J Contemp Brachytherapy. 2023 Dec;15(6):453-464. doi: 10.5114/jcb.2023.133676. Epub 2023 Dec 12. J Contemp Brachytherapy. 2023. PMID: 38230395 Free PMC article.
-
Dose-response relationship between volume base dose and tumor local control in definitive radiotherapy for vaginal cancer.BMC Cancer. 2024 Jun 8;24(1):707. doi: 10.1186/s12885-024-12486-1. BMC Cancer. 2024. PMID: 38851692 Free PMC article.
References
-
- Whitcomb BP. Gynecologic malignancies. Surg Clin North Am 2008; 88: 301-317. - PubMed
-
- Chapman CH, Maghsoudi K, Littell RD et al. . Salvage high-dose-rate brachytherapy and external beam radiotherapy for isolated vaginal recurrences of endometrial cancer with no prior adjuvant therapy. Brachytherapy 2017; 16: 1152-1158. - PubMed
-
- Jhingran A, Burke TW, Eifel PJ. Definitive radiotherapy for patients with isolated vaginal recurrence of endometrial carcinoma after hysterectomy. Int J Radiat Oncol Biol Phys 2003; 56: 1366-1372. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous