

Transvenous lead extraction in a patient with polysplenia and inferior vena cava defect
- PMID: 33437340
- PMCID: PMC7783646
- DOI: 10.1016/j.jccase.2020.09.004
Transvenous lead extraction in a patient with polysplenia and inferior vena cava defect
Abstract
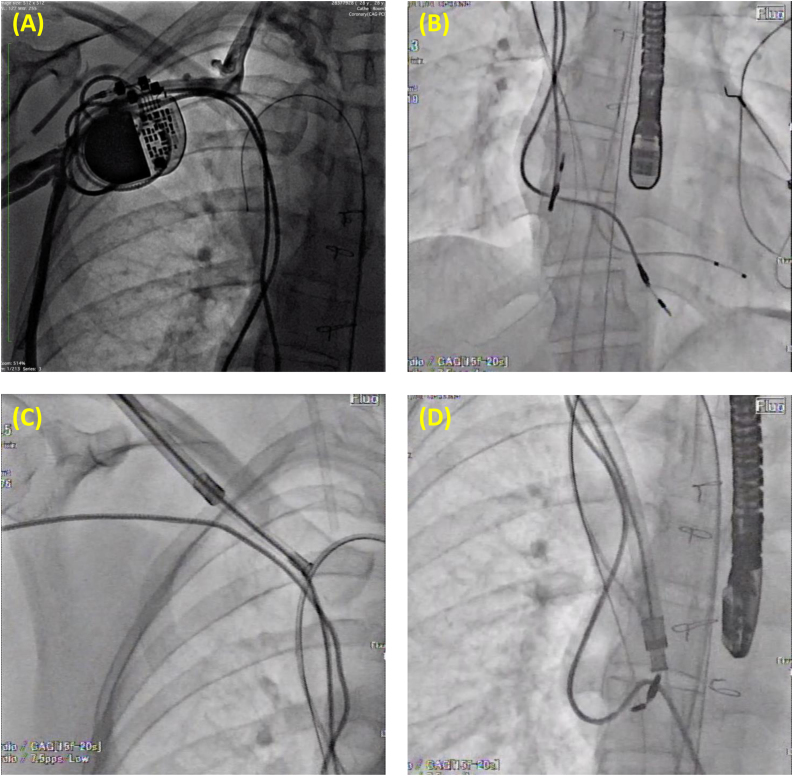
A 28-year-old woman with polysplenia was referred to our hospital for atrial lead failure. She had undergone an intracardiac repair (ICR) for incomplete atrioventricular septal defect and the implantation of epicardial pacing leads due to complete atrioventricular block at the age of 1 year. When she was 13 years old, an endocardial dual-chamber pacemaker was implanted via the right subclavian vein because of epicardial lead failure. The contrast-enhanced computed tomography scan revealed an inferior vena cava defect with an azygos vein connection to the superior vena cava, occlusion of the right brachiocephalic vein, a defect of the left brachiocephalic vein, and a persistent left superior vena cava ligated at the ICR. Therefore, lead exchange was indicated. During the operation, the temporary pacing lead and the guidewire for emergent deployment of the Bridge Occlusion Balloon® were advanced through the azygos vein and placed at the right ventricle and the hepatic vein, respectively. Both 11-Fr and 13-Fr mechanical rotational dilator sheaths were needed for the lead extraction owing to dense calcification and tight adhesions. The atrial lead was successfully extracted without any complications despite extremely restricted venous access. A new atrial lead was inserted through the space created by the 13-Fr sheath. <Learning objective: Transvenous lead extraction in patients with polysplenia is technically challenging. These patients often undergo pacemaker implantation in childhood, which results in tight adhesions and dense calcifications on the leads, and venous access is extremely restricted. It may be impossible to use a snare and deploy the endovascular balloon to prevent a catastrophic complication from the right femoral vein to the superior vena cava in cases of the inferior vena cava defect.>.
Keywords: Congenital heart disease; Inferior vena cava defect; Lead extraction; Pacemaker; Polysplenia.
© 2020 Japanese College of Cardiology. Published by Elsevier Ltd.
Conflict of interest statement
The authors report no declarations of interest.
Figures


Similar articles
-
Successful implantation of a leadless pacemaker in a patient with complete atrioventricular block and congenital absence of superior vena cava: a case report.Eur Heart J Case Rep. 2021 May 12;5(5):ytab167. doi: 10.1093/ehjcr/ytab167. eCollection 2021 May. Eur Heart J Case Rep. 2021. PMID: 34124567 Free PMC article.
-
Permanent pacemaker implantation in a patient with persistent left superior vena cava with an absent right superior vena cava: A case report.J Cardiol Cases. 2020 Dec 11;24(1):34-36. doi: 10.1016/j.jccase.2020.11.024. eCollection 2021 Jul. J Cardiol Cases. 2020. PMID: 34257759 Free PMC article.
-
Complications of permanent cardiac pacing in patients with persistent left superior vena cava.Cardiol J. 2014;21(2):128-37. doi: 10.5603/CJ.a2014.0006. Epub 2014 Feb 14. Cardiol J. 2014. PMID: 24526508
-
Doppler flow velocity patterns of the superior vena cava, inferior vena cava, hepatic vein, coronary sinus, and atrial septal defect: a guide for the echocardiographer.J Am Soc Echocardiogr. 1991 Sep-Oct;4(5):503-12. doi: 10.1016/s0894-7317(14)80386-6. J Am Soc Echocardiogr. 1991. PMID: 1742040 Review.
-
New Insights in Central Venous Disorders. The Role of Transvenous Lead Extractions.Front Cardiovasc Med. 2022 Feb 23;9:783576. doi: 10.3389/fcvm.2022.783576. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35282352 Free PMC article. Review.
Cited by
-
A Rare Entity-Percutaneous Lead Extraction in a Very Late Onset Pacemaker Endocarditis: Case Report and Review of Literature.Diagnostics (Basel). 2021 Jan 9;11(1):96. doi: 10.3390/diagnostics11010096. Diagnostics (Basel). 2021. PMID: 33435384 Free PMC article.
-
Repair of pacemaker lead-induced right ventricular perforation via a left mini-thoracotomy.J Cardiol Cases. 2021 Jun 16;24(6):307-309. doi: 10.1016/j.jccase.2021.05.008. eCollection 2021 Dec. J Cardiol Cases. 2021. PMID: 34917217 Free PMC article.
-
Stepwise transvenous lead extraction due to pacemaker pocket infection following lactational mastitis complicated with breast abscess.Int Breastfeed J. 2024 Apr 19;19(1):27. doi: 10.1186/s13006-024-00633-0. Int Breastfeed J. 2024. PMID: 38641819 Free PMC article.
References
-
- Bongiorni M.G., Kennergren C., Butter C., Deharo J.C., Kutarski A., Rinaldi C.A. The European Lead Extraction ConTRolled (ELECTRa) study: a European Heart Rhythm Association (EHRA) registry of transvenous lead extraction outcomes. Eur Heart J. 2017;38:2995–3005. - PubMed
-
- Gourraud J.B., Chaix M.A., Shohoudi A., Pagé P., Dubuc M., Thibault B. Transvenous lead extraction in adults with congenital heart disease: insights from a 20-year single-center experience. Circ Arrhythm Electrophysiol. 2018;11 - PubMed
-
- Fortescue E.B., Berul C.I., Cecchin F., Walsh E.P., Triedman J.K., Alexander M.E. Patient, procedural, and hardware factors associated with pacemaker lead failures in pediatrics and congenital heart disease. Heart Rhythm. 2004;1:150–159. - PubMed
-
- Atallah J., Erickson C.C., Cecchin F., Dubin A.M., Law I.H., Cohen M.I. Multi-institutional study of implantable defibrillator lead performance in children and young adults: results of the Pediatric Lead Extractability and Survival Evaluation (PLEASE) study. Circulation. 2013;127:2393–2402. - PubMed
-
- Moller J.H., Nakib A., Anderson R.C., Edwards J.E. Congenital cardiac disease associated with polysplenia. A developmental complex of bilateral “left-sidedness.”. Circulation. 1967;36:789–799. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
