

Partial pancreatic tail preserving subtotal pancreatectomy for pancreatic cancer: Improving glycemic control and quality of life without compromising oncological outcomes
- PMID: 33437401
- PMCID: PMC7769744
- DOI: 10.4240/wjgs.v12.i12.491
Partial pancreatic tail preserving subtotal pancreatectomy for pancreatic cancer: Improving glycemic control and quality of life without compromising oncological outcomes
Abstract
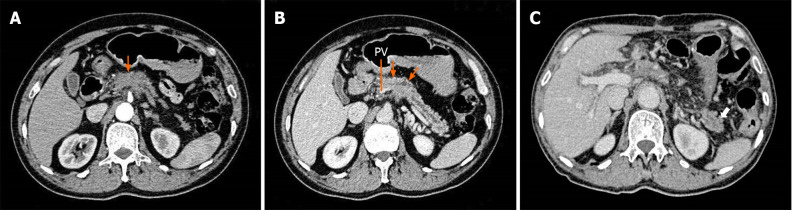
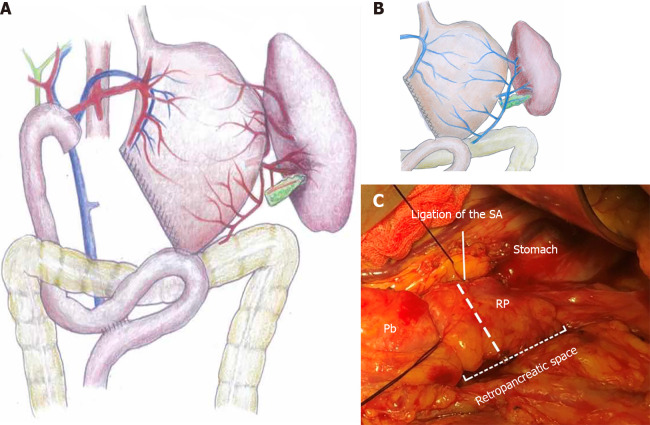
Background: Total pancreatectomy (TP) is usually considered a therapeutic option for pancreatic cancer in which Whipple surgery and distal pancreatectomy are undesirable, but brittle diabetes and poor quality of life (QoL) remain major concerns. A subset of patients who underwent TP even died due to severe hypoglycemia. For pancreatic cancer involving the pancreatic head and proximal body but without invasion to the pancreatic tail, we performed partial pancreatic tail preserving subtotal pancreatectomy (PPTP-SP) in selected patients, in order to improve postoperative glycemic control and QoL without compromising oncological outcomes.
Aim: To evaluate the efficacy of PPTP-SP for patients with pancreatic cancer.
Methods: We retrospectively reviewed 56 patients with pancreatic ductal adenocarcinoma who underwent PPTP-SP (n = 18) or TP (n = 38) at our institution from May 2014 to January 2019. Clinical outcomes were compared between the two groups, with an emphasis on oncological outcomes, postoperative glycemic control, and QoL. QoL was evaluated using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30 and EORTC PAN26). All patients were followed until May 2019 or until death.
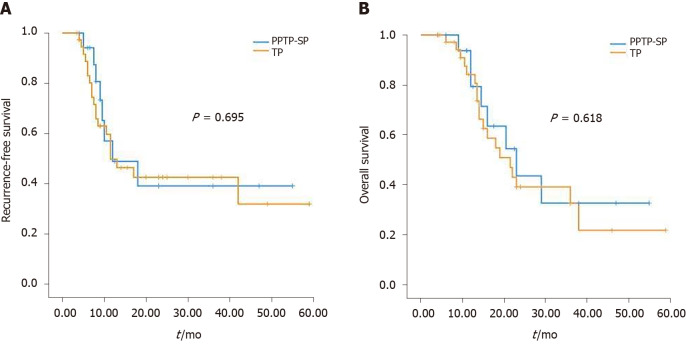
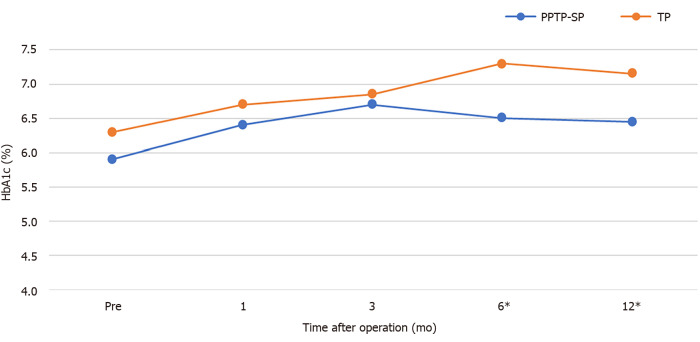
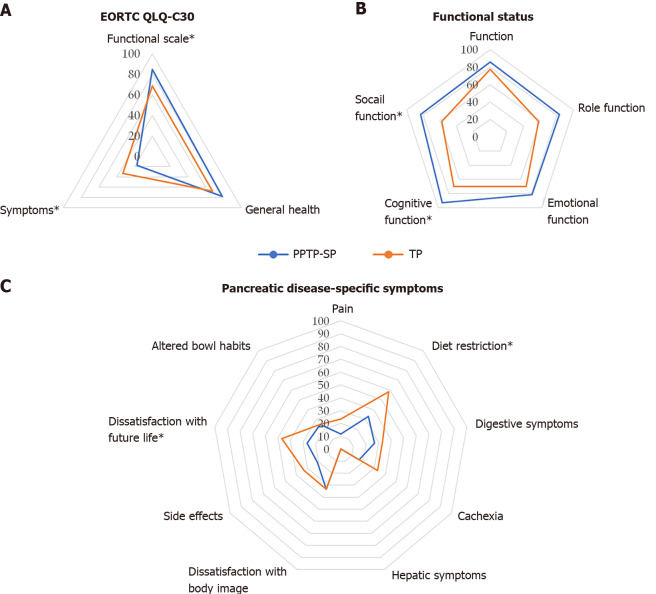
Results: A total of 56 consecutive patients were enrolled in this study. Perioperative outcomes, recurrence-free survival, and overall survival were comparable between the two groups. No patients in the PPTP-SP group developed cancer recurrence in the pancreatic tail stump or splenic hilum, or a clinical pancreatic fistula. Patients who underwent PPTP-SP had significantly better glycemic control, based on their higher rate of insulin-independence (P = 0.014), lower hemoglobin A1c (HbA1c) level (P = 0.046), lower daily insulin dosage (P < 0.001), and less frequent hypoglycemic episodes (P < 0.001). Global health was similar in the two groups, but patients who underwent PPTP-SP had better functional status (P = 0.036), milder symptoms (P = 0.013), less severe diet restriction (P = 0.011), and higher confidence regarding future life (P = 0.035).
Conclusion: For pancreatic cancer involving the pancreatic head and proximal body, PPTP-SP achieves perioperative and oncological outcomes comparable to TP in selected patients while significantly improving long-term glycemic control and QoL.
Keywords: Diabetes mellitus; Pancreatic cancer; Partial pancreatic tail preserving subtotal pancreatectomy; Quality of life; Total pancreatectomy; Treatment outcome.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: We declare that we have no conflicts of interest related to this study.
Figures
Similar articles
-
Quality of life in patients after total pancreatectomy is comparable with quality of life in patients who undergo a partial pancreatic resection.J Surg Res. 2014 Mar;187(1):189-96. doi: 10.1016/j.jss.2013.10.004. Epub 2013 Oct 9. J Surg Res. 2014. PMID: 24411300
-
Pylorus-preserving total pancreatectomy for pancreatic cancer.World J Surg. 2000 Jan;24(1):66-70; discussion 70-1. doi: 10.1007/s002689910013. World J Surg. 2000. PMID: 10594206
-
Is there still a role for total pancreatectomy?Ann Surg. 2007 Dec;246(6):966-74; discussion 974-5. doi: 10.1097/SLA.0b013e31815c2ca3. Ann Surg. 2007. PMID: 18043098
-
Perioperative management of endocrine insufficiency after total pancreatectomy for neoplasia.Langenbecks Arch Surg. 2017 Sep;402(6):873-883. doi: 10.1007/s00423-017-1603-8. Epub 2017 Jul 21. Langenbecks Arch Surg. 2017. PMID: 28733926 Review.
-
The Clinical Outcomes after Total Pancreatectomy.Dig Surg. 2017;34(2):142-150. doi: 10.1159/000449234. Epub 2016 Oct 5. Dig Surg. 2017. PMID: 27701159 Review.
Cited by
-
Laparoscopic Duodenum and Spleen-Preserving Subtotal or Total Pancreatectomy: A Parenchyma-Sparing Strategy for Main Duct Intraductal Papillary Mucinous Neoplasms (with Video).Ann Surg Oncol. 2024 Dec;31(13):8734-8740. doi: 10.1245/s10434-024-16244-2. Epub 2024 Sep 23. Ann Surg Oncol. 2024. PMID: 39312053 Free PMC article.
-
Global status of research on gastrointestinal cancer patients' quality of life: A bibliometric and visual analysis from 2003 to 2023.Heliyon. 2023 Dec 6;10(1):e23377. doi: 10.1016/j.heliyon.2023.e23377. eCollection 2024 Jan 15. Heliyon. 2023. PMID: 38148818 Free PMC article.
References
LinkOut - more resources
Full Text Sources
