

Which is the most effective treatment for lumbar spinal stenosis: Decompression, fusion, or interspinous process device? A Bayesian network meta-analysis
- PMID: 33437622
- PMCID: PMC7773978
- DOI: 10.1016/j.jot.2020.07.003
Which is the most effective treatment for lumbar spinal stenosis: Decompression, fusion, or interspinous process device? A Bayesian network meta-analysis
Abstract
Objective: To compare the clinical efficacy, complications, and reoperation rates among three major treatments for lumbar spinal stenosis (LSS): decompression, fusion, and interspinous process device (IPD), using a Bayesian network meta-analysis.
Materials and methods: Databases including Pubmed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science were used for the literature search. Randomized Controlled Trials (RCTs) with three treatment methods were reviewed and included in the study. R software (version 3.6.0), Stata (version 14.0), and Review Manager (version 5.3) were used to perform data analysis.
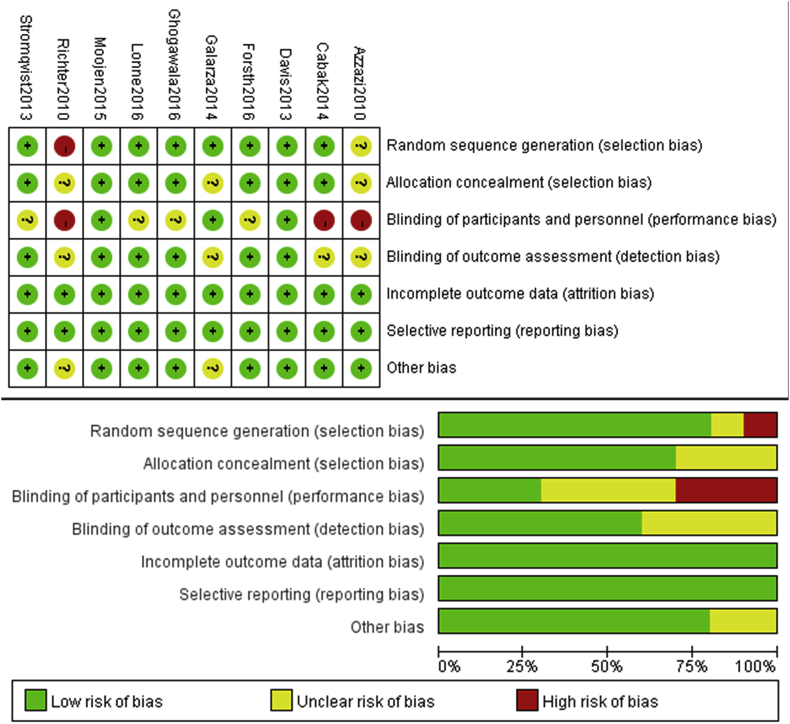
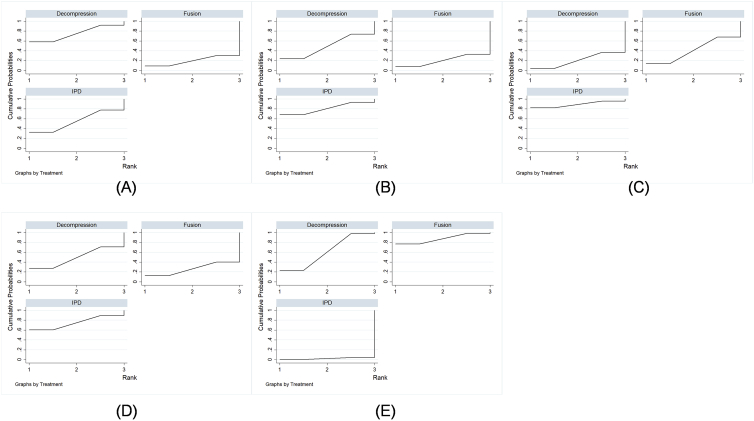
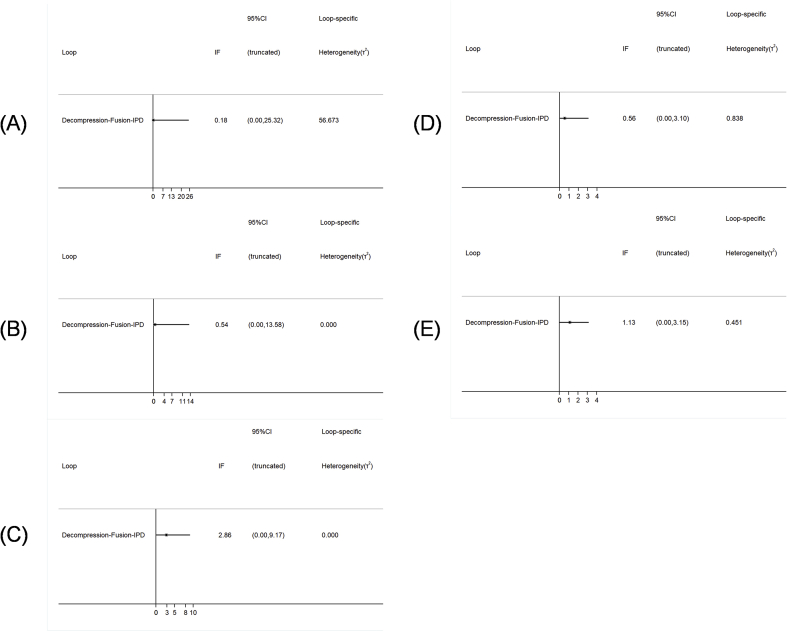
Results: A total of 10 RCTs involving 1254 patients were enrolled in the present study and each study met an acceptable quality according to our quality assessment described later. In direct comparison, IPD exhibited a higher incidence of reoperation than fusion (OR = 2.93, CI: 1.07-8.02). In indirect comparison, the rank of VAS leg (from best to worst) was as follows: IPD (64%) > decompression (25%) > fusion (11%), and the rank of ODI (from best to worst) was: IPD (84%) > fusion (13%) > decompression (4%). IPD had the lowest incidence of complications; the rank of complications (from best to worst) was: IPD (60%) > decompression (27%) > fusion (14%). However, for the rank of reoperation, fusion showed the best results (from best to worst): fusion (79%) > decompression (20%) > IPD (1%). Consistency tests at global and local level showed satisfactory results and heterogeneity tests using loop text indicated a favorable stability.
Conclusion: The present study preliminarily indicates that non-fusion methods including decompression and IPD are optimal choices for treating LSS, which achieves favorable clinical outcomes. IPD exhibits a low incidence of complications, but its high rate of reoperation should be treated with caution.
The translational potential of this article: For the treatment of LSS, several procedures including decompression, fusion, and IPD have been reported. However, each method has its own advantages and disadvantages. To date, the golden standard treatment for LSS is still controversial. In this network meta-analysis, our results demonstrate that both decompression and IPD obtain satisfactory clinical effects for LSS. IPD is accompanied with a low incidence of complications, however, its high rate of reoperation should be acknowledged with discretion.
Keywords: Decompression; Fusion; IPD, interspinous process device; Interspinous process device; LSS, lumbar spinal stenosis; Lumbar spinal stenosis; Network meta-analysis; ODI, oswestry disability index; VAS, visual analogue scale.
© 2020 The Authors.
Conflict of interest statement
The authors have no conflicts of interest to disclose in relation to this article.
Figures








Similar articles
-
Comparison of the efficacy and safety between interspinous process distraction device and open decompression surgery in treating lumbar spinal stenosis: a meta analysis.J Invest Surg. 2015 Feb;28(1):40-9. doi: 10.3109/08941939.2014.932474. Epub 2014 Jul 15. J Invest Surg. 2015. PMID: 25025237
-
Efficacy and safety of interspinous process device compared with alone decompression for lumbar spinal stenosis: A systematic review and meta-analysis.Medicine (Baltimore). 2024 Jun 7;103(23):e38370. doi: 10.1097/MD.0000000000038370. Medicine (Baltimore). 2024. PMID: 38847722 Free PMC article.
-
Decompression Surgery versus Interspinous Devices for Lumbar Spinal Stenosis: A Systematic Review of the Literature.Asian Spine J. 2020 Aug;14(4):526-542. doi: 10.31616/asj.2019.0105. Epub 2020 Jan 8. Asian Spine J. 2020. PMID: 31906617 Free PMC article.
-
Interspinous process spacers versus traditional decompression for lumbar spinal stenosis: systematic review and meta-analysis.J Spine Surg. 2016 Mar;2(1):31-40. doi: 10.21037/jss.2016.01.07. J Spine Surg. 2016. PMID: 27683693 Free PMC article.
-
Fusion or Not for Degenerative Lumbar Spinal Stenosis: A Meta-Analysis and Systematic Review.Pain Physician. 2018 Jan;21(1):1-8. Pain Physician. 2018. PMID: 29357326
Cited by
-
Lumbar Stenosis Spinal Surgery-Associated Cerebrospinal Fluid Leak Without Headache: An Autobiographical Case Report.Cureus. 2022 May 23;14(5):e25253. doi: 10.7759/cureus.25253. eCollection 2022 May. Cureus. 2022. PMID: 35755552 Free PMC article.
-
Unilateral biportal endoscopic transforaminal lumbar interbody fusion versus conventional interbody fusion for the treatment of degenerative lumbar spine disease: a systematic review and meta-analysis.BMC Musculoskelet Disord. 2023 Oct 24;24(1):838. doi: 10.1186/s12891-023-06949-y. BMC Musculoskelet Disord. 2023. PMID: 37875873 Free PMC article.
-
Unilateral biportal endoscopic lumbar interbody fusion vs. posterior lumbar interbody fusion for the treatment of bilateral lumbar spinal stenosis.Front Surg. 2025 Jun 30;12:1533458. doi: 10.3389/fsurg.2025.1533458. eCollection 2025. Front Surg. 2025. PMID: 40661157 Free PMC article.
-
The Fusion Rate of Cortical Bone Trajectory Screw Fixation and Pedicle Screw Fixations in L4-5 Interbody Fusion: A Retrospective Cohort Study.Orthop Surg. 2023 May;15(5):1281-1288. doi: 10.1111/os.13704. Epub 2023 Apr 18. Orthop Surg. 2023. PMID: 37073082 Free PMC article.
-
A Biomechanical Evaluation of a Novel Interspinous Process Device: In Vitro Flexibility Assessment and Finite Element Analysis.Bioengineering (Basel). 2025 Apr 3;12(4):384. doi: 10.3390/bioengineering12040384. Bioengineering (Basel). 2025. PMID: 40281744 Free PMC article.
References
-
- Thomas K., Faris P., McIntosh G., Manners S., Abraham E., Bailey C.S. Decompression alone vs. decompression plus fusion for claudication secondary to lumbar spinal stenosis. Spine J. 2019;19(10):1633–1639. - PubMed
-
- Lee C.H., Hyun S.J., Kim K.J., Jahng T.A., Yoon S.H., Kim H.J. The efficacy of lumbar hybrid stabilization using the DIAM to delay adjacent segment degeneration: an intervention comparison study with a minimum 2-year follow-up. Neurosurgery. 2013;73(2 Suppl Operative) ons224-231; discussion ons231-222. - PubMed
-
- Ahmad S., Hamad A., Bhalla A., Turner S., Balain B., Jaffray D. The outcome of decompression alone for lumbar spinal stenosis with degenerative spondylolisthesis. Eur Spine J. 2017;26(2):414–419. - PubMed
-
- Masuda S., Kanba Y., Kawai J., Ikeda N. Outcomes after decompression surgery without fusion for patients with lumbar spinal stenosis and substantial low back pain. Eur Spine J. 2019;29(1):147–152. - PubMed
-
- Ng K.K.M., Cheung J.P.Y. Is minimally invasive surgery superior to open surgery for treatment of lumbar spinal stenosis? A systematic review. J Orthop Surg. 2017;25(2) 2309499017716254. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
