

Exocrine drainage in pancreas transplantation: Complications and management
- PMID: 33437672
- PMCID: PMC7769732
- DOI: 10.5500/wjt.v10.i12.392
Exocrine drainage in pancreas transplantation: Complications and management
Abstract
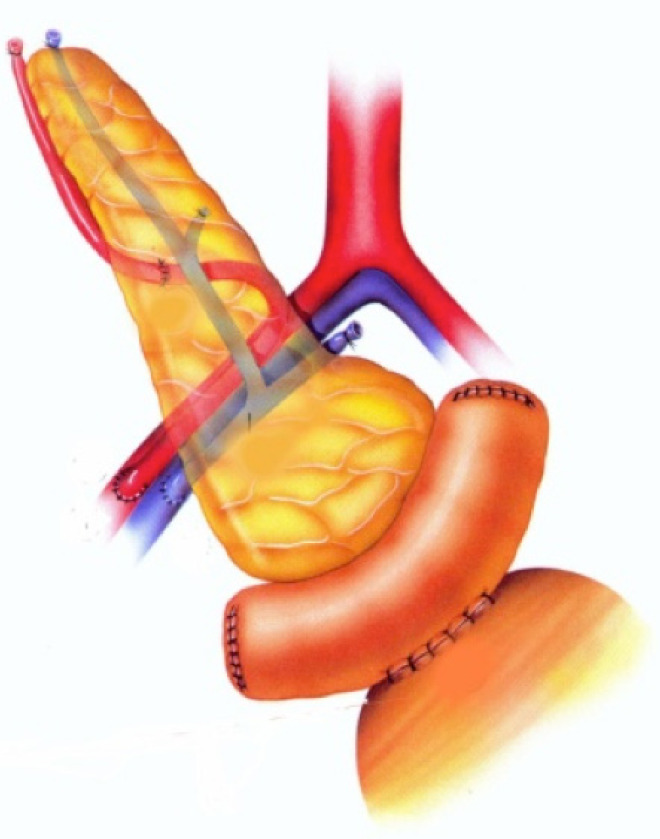
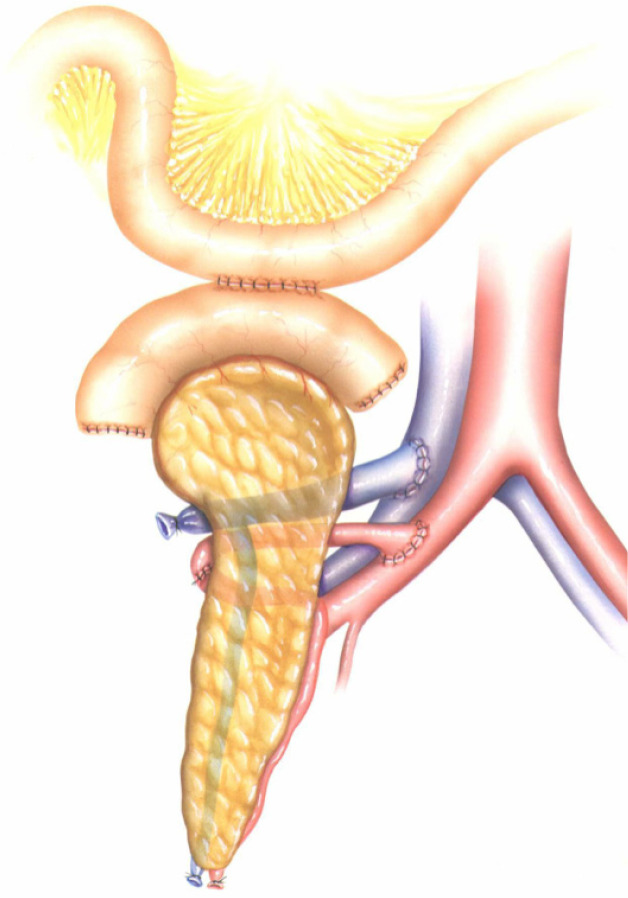
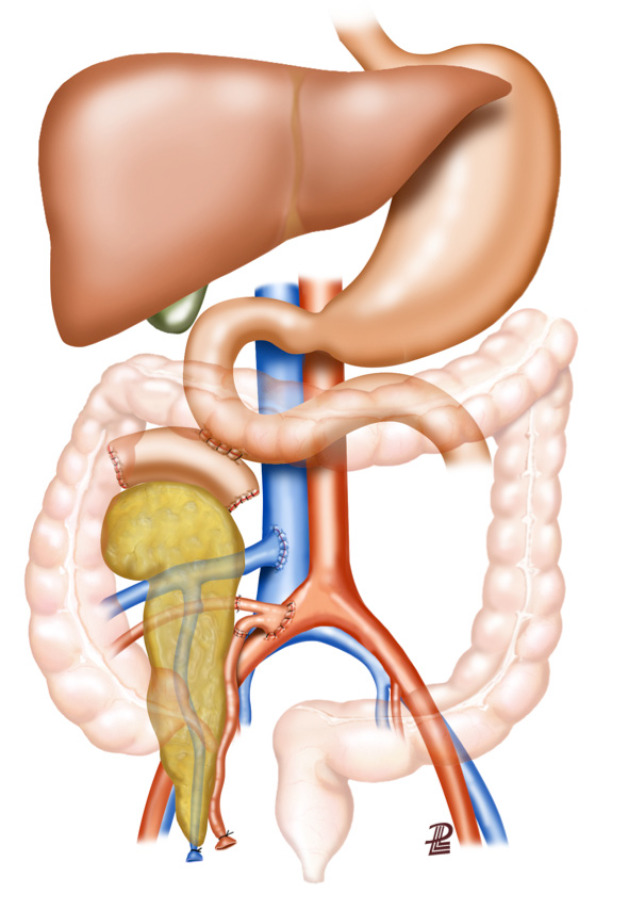
The aim of this minireview is to compare various pancreas transplantation exocrine drainage techniques i.e., bladder vs enteric. Both techniques have different difficulties and complications. Numerous comparisons have been made in the literature between exocrine drainage techniques throughout the history of pancreas transplantation, detailing complications and their impact on graft and patient survival. Specific emphasis has been made on the early postoperative management of these complications and the related surgical infections and their consequences. In light of the results, a number of bladder-drained pancreas grafts required conversion to enteric drainage. As a result of technical improvements, outcomes of the varied enteric exocrine drainage techniques (duodenojejunostomy, duodenoduodenostomy or gastric drainage) have also been discussed i.e., assessing specific risks vs benefits. Pancreatic exocrine secretions can be drained to the urinary or intestinal tracts. Until the late 1990s the bladder drainage technique was used in the majority of transplant centers due to ease of monitoring urine amylase and lipase levels for evaluation of possible rejection. Moreover, bladder drainage was associated at that time with fewer surgical complications, which in contrast to enteric drainage, could be managed with conservative therapies. Nowadays, the most commonly used technique for proper driving of exocrine pancreatic secretions is enteric drainage due to the high rate of urological and metabolic complications associated with bladder drainage. Of note, 10% to 40% of bladder-drained pancreata eventually required enteric conversion at no detriment to overall graft survival. Various surgical techniques were originally described using the small bowel for enteric anastomosis with Roux-en-Y loop or a direct side-to-side anastomosis. Despite the improvements in surgery, enteric drainage complication rates ranging from 2%-20% have been reported. Treatment depends on the presence of any associated complications and the condition of the patient. Intra-abdominal infection represents a potentially very serious problem. Up to 30% of deep wound infections are associated with an anastomotic leak. They can lead not only to high rates of graft loss, but also to substantial mortality. New modifications of established techniques are being developed, such as gastric or duodenal exocrine drainage. Duodenoduodenostomy is an interesting option, in which the pancreas is placed behind the right colon and is oriented cephalad. The main concern of this technique is the challenge of repairing the native duodenum when allograft pancreatectomy is necessary. Identification and prevention of technical failure remains the main objective for pancreas transplantation surgeons. In conclusion, despite numerous techniques to minimize exocrine pancreatic drainage complications e.g., leakage and infection, no universal technique has been standardized. A prospective study/registry analysis may resolve this.
Keywords: Anastomotic leak; Graft survival; Infection; Morbidity; Patient survival; Surgery.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Conversion of exocrine secretions from bladder to enteric drainage in recipients of whole pancreaticoduodenal transplants.Ann Surg. 1992 Dec;216(6):663-72. doi: 10.1097/00000658-199212000-00008. Ann Surg. 1992. PMID: 1466620 Free PMC article.
-
Exocrine drainage in vascularized pancreas transplantation in the new millennium.World J Transplant. 2016 Jun 24;6(2):255-71. doi: 10.5500/wjt.v6.i2.255. World J Transplant. 2016. PMID: 27358771 Free PMC article. Review.
-
Conversion from bladder to enteric drainage after pancreaticoduodenal transplantations.Surgery. 1998 Nov;124(5):883-93. Surgery. 1998. PMID: 9823403
-
Urological complications and enteric conversion after pancreas transplantation with bladder drainage.Transplant Proc. 1994 Apr;26(2):458-9. Transplant Proc. 1994. PMID: 8171502
-
Bladder vs enteric drainage following pancreatic transplantation: How best to support graft survival? A best evidence topic.Int J Surg. 2015 Oct;22:149-52. doi: 10.1016/j.ijsu.2015.08.072. Epub 2015 Sep 3. Int J Surg. 2015. PMID: 26343973 Review.
Cited by
-
Retroperitoneal pancreas transplantation with a Roux-en-Y duodenojejunostomy for exocrine drainage.BMC Surg. 2024 Nov 13;24(1):357. doi: 10.1186/s12893-024-02658-y. BMC Surg. 2024. PMID: 39538165 Free PMC article.
-
Multimodality diagnostic imaging and role of interventional radiology in pancreas transplantation.Abdom Radiol (NY). 2025 May 29. doi: 10.1007/s00261-025-05003-w. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40439720 Review.
-
Current Trends in Organ Preservation Solutions for Pancreas Transplantation: A Single-Center Retrospective Study.Transpl Int. 2022 Mar 28;35:10419. doi: 10.3389/ti.2022.10419. eCollection 2022. Transpl Int. 2022. PMID: 35418805 Free PMC article.
-
Delivery of therapeutic agents and cells to pancreatic islets: Towards a new era in the treatment of diabetes.Mol Aspects Med. 2022 Feb;83:101063. doi: 10.1016/j.mam.2021.101063. Epub 2021 Dec 24. Mol Aspects Med. 2022. PMID: 34961627 Free PMC article. Review.
-
Whole-Organ Pancreas and Islets Transplantations in UK: An Overview and Future Directions.J Clin Med. 2023 May 1;12(9):3245. doi: 10.3390/jcm12093245. J Clin Med. 2023. PMID: 37176684 Free PMC article. Review.
References
-
- Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967;61:827–837. - PubMed
-
- Di Carlo V, Castoldi R, Cristallo M, Ferrari G, Socci C, Baldi A, Molteni B, Secchi A, Pozza G. Techniques of pancreas transplantation through the world: an IPITA Center survey. Transplant Proc. 1998;30:231–241. - PubMed
-
- Laftavi MR, Gruessner A, Gruessner R. Surgery of pancreas transplantation. Curr Opin Organ Transplant. 2017;22:389–397. - PubMed
-
- Sutherland DE, Gruessner RW, Gruessner AC. Pancreas transplantation for treatment of diabetes mellitus. World J Surg. 2001;25:487–496. - PubMed
-
- West M, Gruessner AC, Metrakos P, Sutherland DE, Gruessner RW. Conversion from bladder to enteric drainage after pancreaticoduodenal transplantations. Surgery. 1998;124:883–893. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
