

Direct admission to improve timely access to care for patients requiring transfer to a level 1 trauma center
- PMID: 33437873
- PMCID: PMC7780511
- DOI: 10.1136/tsaco-2020-000607
Direct admission to improve timely access to care for patients requiring transfer to a level 1 trauma center
Abstract
Background: Emergency departments (EDs) at level 1 trauma centers are often overcrowded and deny ED-to-ED transfers from lower-tiered centers. Lack of access to timely level 1 care is associated with increased mortality. We evaluated the feasibility of a direct admission (DA) protocol as a method to increase timely access to a level 1 trauma center during periods of ED overcrowding.
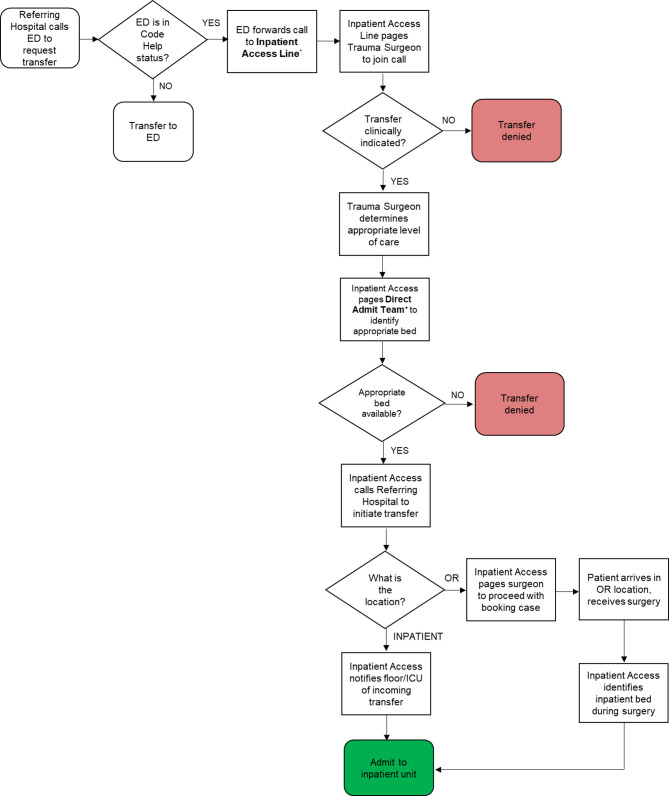
Methods: During periods of ED overcrowding between 1 May and 31 December 2019, we admitted patients from referring EDs directly to the intensive care unit (ICU) or inpatient ward using the DA protocol. In a prospective comparative study design, we compared their outcomes to patients during the same period who were admitted through the ED when the ED was not overcrowded.
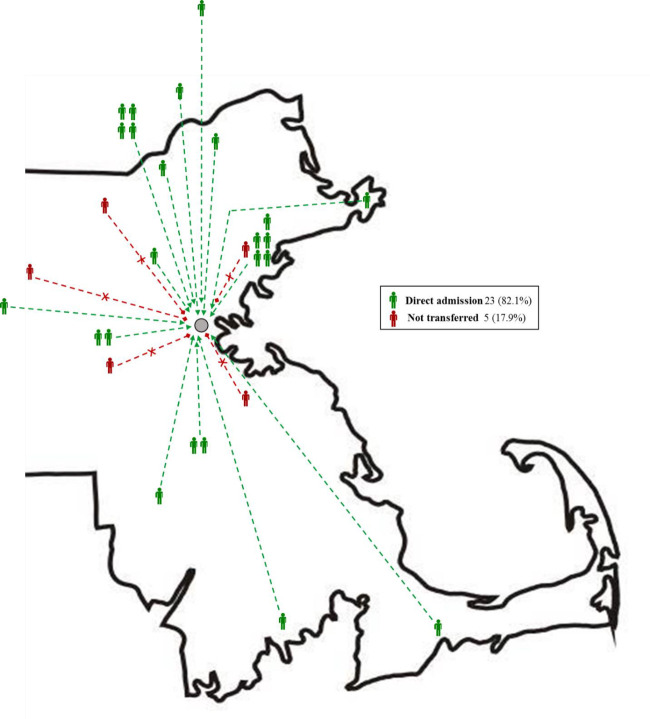
Results: During periods of ED overcrowding, transfer was requested and clinically accepted for 28 patients, of which 23 (82.1%, age 63±20.3 years, men 52.2% men) were successfully admitted via the DA protocol. Five (17.9%) were not successfully transferred due to lack of available inpatient beds. During periods when the ED was not overcrowded, 106 patients (age 62.8±23.1 years, men 52.8%) were admitted via the ED. There were no morbidity or mortality events attributed to the DA process. Time to patient arrival was 2.7 hours (95% CI 2.3 to 3.1) in the DA cohort and 1.9 hours (95% CI 1.5 to 2.4) in the ED-to-ED cohort (p=0.104). Up-triage to the ICU within 24 hours was performed in only one patient (4.3%). In-hospital mortality did not differ (3 (13%) vs. 8 (7.6%), p=0.392).
Discussion: The DA pathway is a feasible method to safely transfer patients from a referring ED to a higher-care trauma center when its ED is overcrowded.
Level of evidence: Level III, care management.
Keywords: access; and evaluation; emergency treatment; healthcare quality; multiple trauma.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Factors associated with the disposition of severely injured patients initially seen at non–trauma center emergency departments: disparities by insurance status.JAMA Surg. 2014 May;149(5):422-30. doi: 10.1001/jamasurg.2013.4398. JAMA Surg. 2014. PMID: 24554059 Free PMC article.
-
Patients admitted via the emergency department to the intensive care unit: An observational cohort study.Emerg Med Australas. 2019 Apr;31(2):225-233. doi: 10.1111/1742-6723.13123. Epub 2018 Jul 11. Emerg Med Australas. 2019. PMID: 29998569
-
The impact of implementing a 24/7 open trauma bed protocol in the surgical intensive care unit on throughput and outcomes.J Trauma Acute Care Surg. 2013 Jul;75(1):97-101. doi: 10.1097/TA.0b013e31829849e5. J Trauma Acute Care Surg. 2013. PMID: 23778446
-
The role of full capacity protocols on mitigating overcrowding in EDs.Am J Emerg Med. 2012 Mar;30(3):412-20. doi: 10.1016/j.ajem.2010.12.035. Epub 2011 Mar 1. Am J Emerg Med. 2012. PMID: 21367554 Review.
-
Pediatric observation status beds on an inpatient unit: an integrated care model.Pediatr Emerg Care. 2004 Jan;20(1):17-21. doi: 10.1097/01.pec.0000106238.72265.5f. Pediatr Emerg Care. 2004. PMID: 14716160 Review.
Cited by
-
Prolonged Length of Stay at Out-Of-State Trauma Centers: Potential Role for Repatriation.J Am Coll Surg. 2025 May 16:10.1097/XCS.0000000000001449. doi: 10.1097/XCS.0000000000001449. Online ahead of print. J Am Coll Surg. 2025. PMID: 40377283
References
LinkOut - more resources
Full Text Sources
Research Materials