

Education, biological ageing, all-cause and cause-specific mortality and morbidity: UK biobank cohort study
- PMID: 33437953
- PMCID: PMC7788440
- DOI: 10.1016/j.eclinm.2020.100658
Education, biological ageing, all-cause and cause-specific mortality and morbidity: UK biobank cohort study
Abstract
Background: Socioeconomic position as measured by education may be embodied and affect the functioning of key physiological systems. Links between social disadvantage, its biological imprint, and cause-specific mortality and morbidity have not been investigated in large populations, and yet may point towards areas for public health interventions beyond targeting individual behaviours.
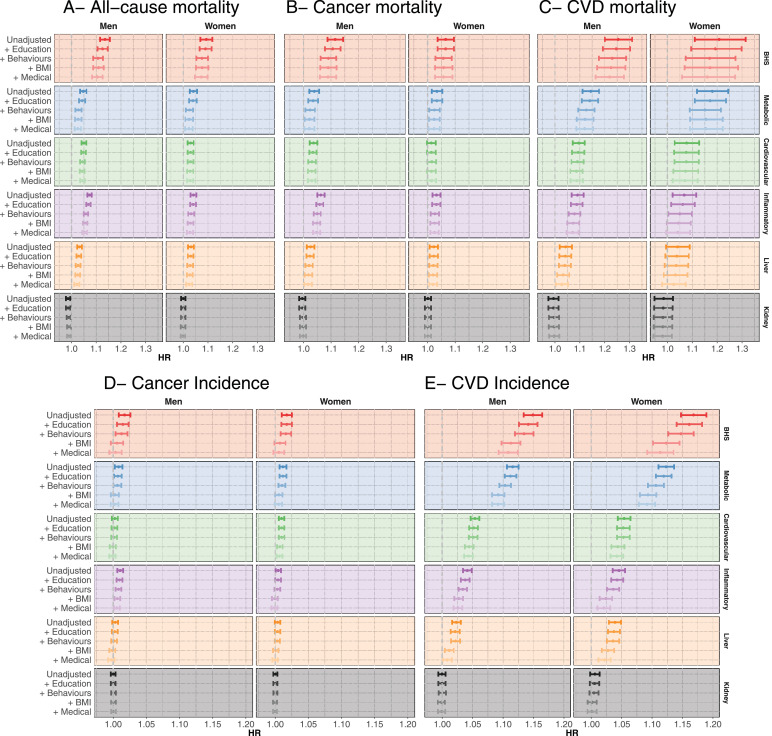
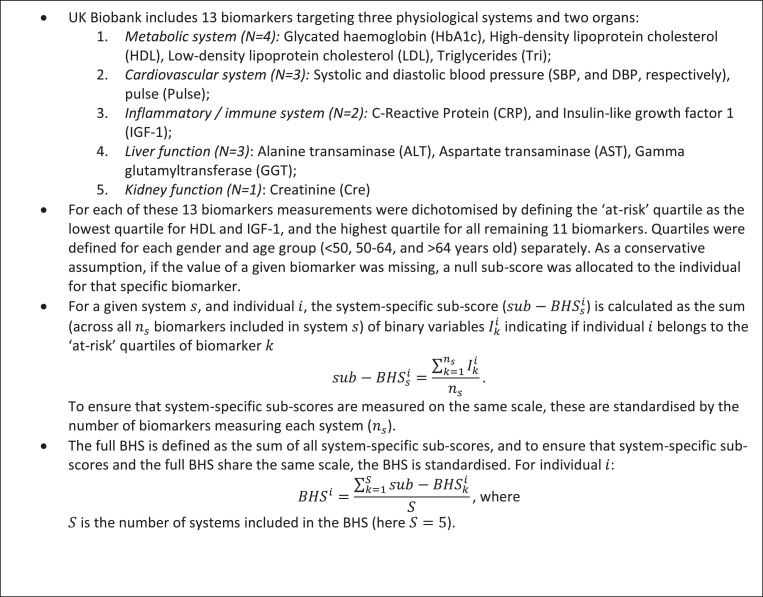
Methods: Using data from 366,748 UK Biobank participants with 13 biomarker measurements, we calculated a Biological Health Score (BHS, ranging from 0 to 1) capturing the level of functioning of five physiological systems. Associations between BHS and incidence of cardiovascular disease (CVD) and cancer, and mortality from all, CVD, cancer, and external causes were examined. We explored the role of education in these associations. Mendelian randomisation using genetic evidence was used to triangulate these findings.
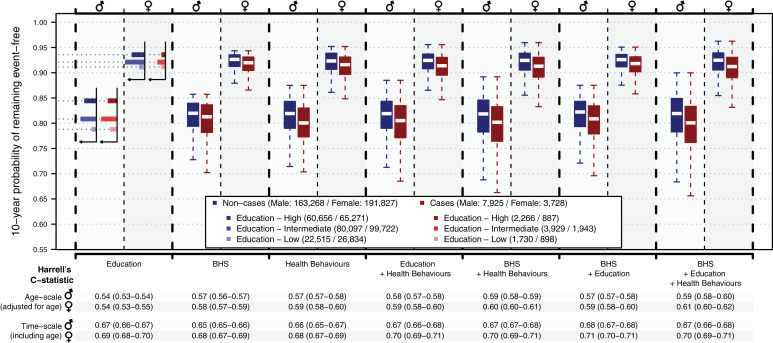
Findings: An increase in BHS of 0.1 was associated with all-cause (HR = 1.14 [1.12-1.16] and 1.09 [1.07-1.12] in men and women respectively), cancer (HR = 1.11 [1.09-1.14] and 1.07 [1.04-1.10]) and CVD (HR = 1.25 [1.20-1.31] and 1.21 [1.11-1.31]) mortality, CVD incidence (HR = 1.15 [1.13-1.16] and 1.17 [1.15-1.19]). These associations survived adjustment for education, lifestyle-behaviours, body mass index (BMI), co-morbidities and medical treatments. Mendelian randomisation further supported the link between the BHS and CVD incidence (HR = 1.31 [1.21-1.42]). The BHS contributed to CVD incidence prediction (age-adjusted C-statistic = 0.58), other than through education and health behaviours.
Interpretation: The BHS captures features of the embodiment of education, health behaviours, and more proximal unknown factors which all complementarily contribute to all-cause, cancer and CVD morbidity and premature death.
Keywords: Allostatic load mortality; Biological ageing; Biomarkers; Incidentpathologies; Mendelian randomisation; Prospective cohort; Social embedding; Uk biobank.
© 2020 The Author(s).
Conflict of interest statement
Prof. Elliott is the director of the MRC Centre of Environment and Health (MR/L01341X/1 and MC/S019669/1) and has no conflict of interest to disclose. Prof Kivimäki reports grants from the Medical Research Council (MR/R024227/1), National Institute on ageing (NIA), US (R01AG056477), Academy of Finland (311,492) and Helsinki Institute of Life Science, outside the submitted work. All other authors do not have any interests to disclose.
Figures


References
-
- Hertzman C. Health and Human Society: wealthier nations are not always healthier, and efforts to improve health can be swamped by the effects of inequality and conflict. Am. Sci. 2001;89(6):538–545.
-
- Foster H.M.E., Celis-Morales C.A., Nicholl B.I. The effect of socioeconomic deprivation on the association between an extended measurement of unhealthy lifestyle factors and health outcomes: a prospective analysis of the UK Biobank cohort. The Lancet Public Health. 2018;3(12):e576–ee85. - PubMed
-
- Petrovic D., de Mestral C., Bochud M. The contribution of health behaviors to socioeconomic inequalities in health: a systematic review. Prev Med. 2018;113:15–31. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
