

Racial Disparities in the Use of Surgical Procedures in the US
- PMID: 33439237
- PMCID: PMC7807389
- DOI: 10.1001/jamasurg.2020.6257
Racial Disparities in the Use of Surgical Procedures in the US
Abstract
Importance: The largest US federal action plan to date for reducing racial disparities in health care was implemented in 2011 and continues today. It is not known whether this program, along with other initiatives, is associated with a decrease in racial disparities in the use of major surgical procedures in the US.
Objective: To analyze whether national initiatives are associated with improvement in racial disparities between White and Black patients in the use of surgical procedures in the US.
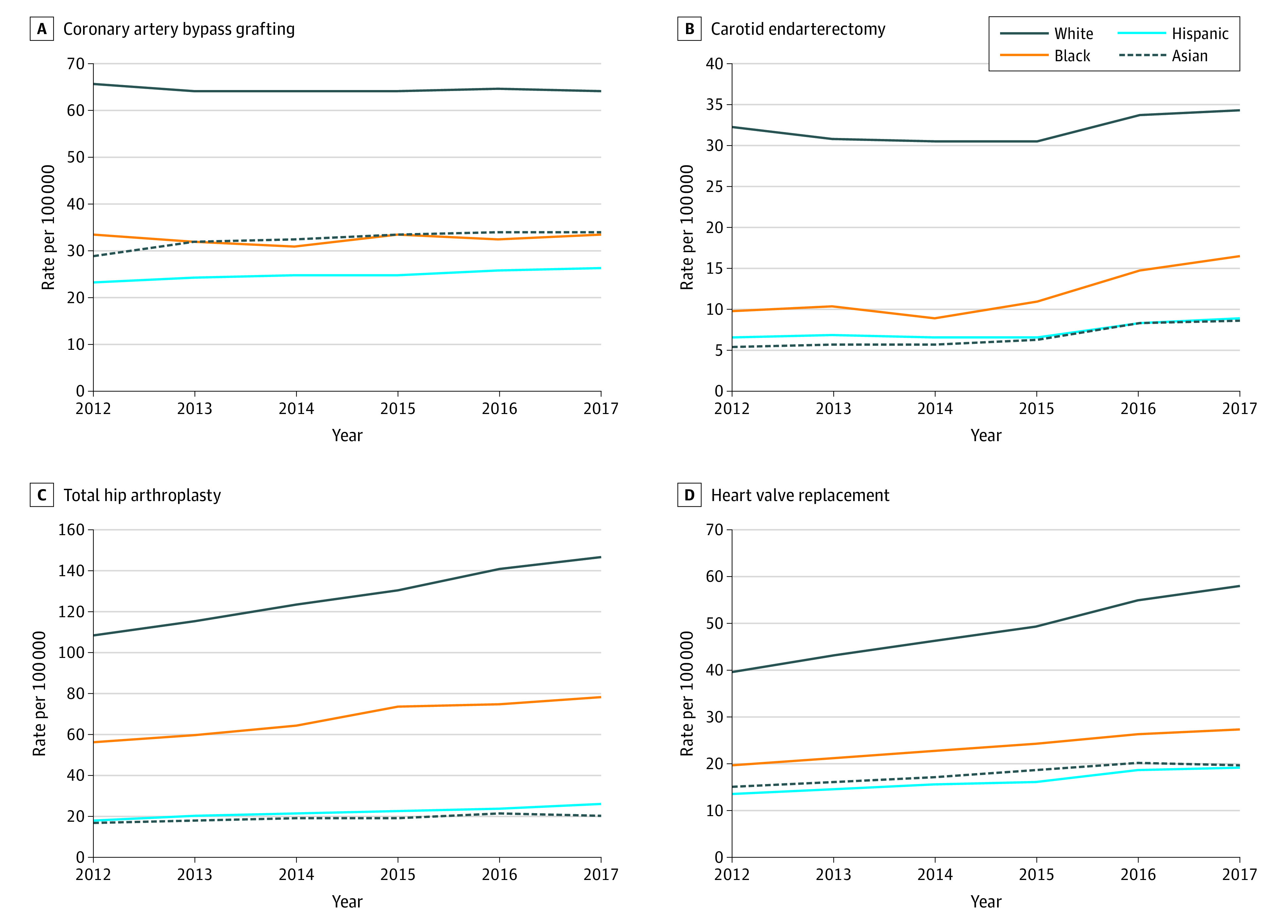
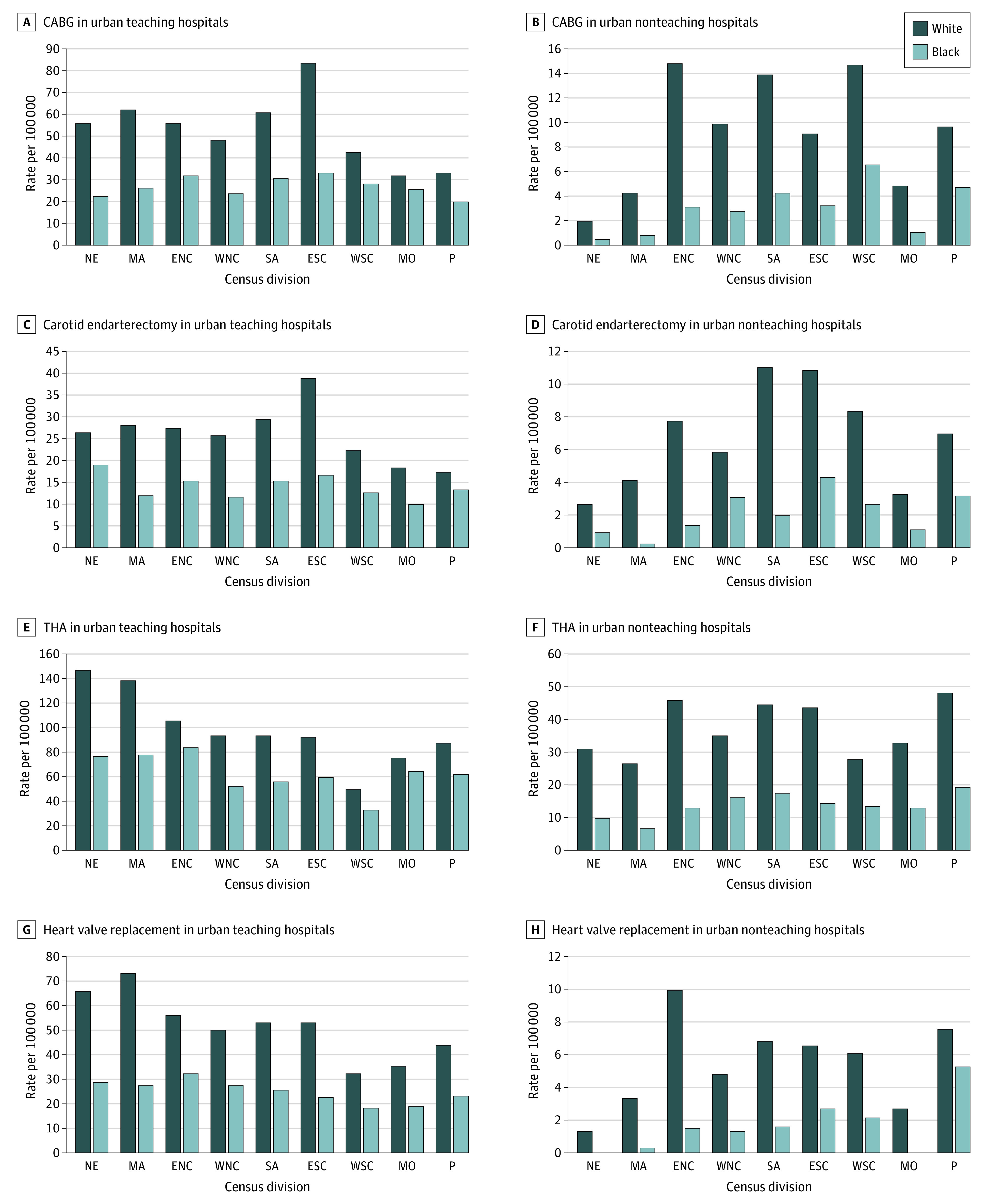
Design, setting, and participants: In this case-control study, the national rates of use for 9 major surgical procedures previously shown to have racial disparities in rates of performance between White and Black adult patients (including angioplasty, spinal fusion, carotid endarterectomy, appendectomy, colorectal resection, coronary artery bypass grafting, total hip arthroplasty, total knee arthroplasty, and heart valve replacement) were analyzed from January 1, 2012, through December 31, 2017. Data analysis was conducted from May 1 to June 30, 2020. Population- and sex-adjusted procedural rates during the study period were examined and standardized based on all-payer insurance status. Racial changes were further analyzed by US census division and hospital teaching status for 4 selected procedures: coronary artery bypass grafting, carotid endarterectomy, total hip arthroplasty, and heart valve replacement.
Main outcomes and measures: Population- and race-adjusted procedural rates by year, US census division, hospital teaching status, and insurance status.
Results: This study included national inpatient data from 2012 to 2017. In 2012, the national incidence rate of all 9 major surgical procedures was higher in White than in Black individuals. For example, the incidence rate of total knee arthroplasty in 2012 for White males was 184.8 per 100 000 persons and for Black males was 79.8 per 100 000 persons. By 2017, these racial disparities persisted for all 9 procedures analyzed. For example, the incidence rate of total knee arthroplasty in 2017 for White males was 220.5 per 100 000 persons and for Black males was 95.6 per 100 000 persons. Although the disparity gap between White and Black patients narrowed for angioplasty (-20.1 per 100 000 persons in males, -4.2 per 100 000 persons in females), spinal fusion (-7.7 per 100 000 persons in males, -15.0 per 100 000 persons in females), carotid endarterectomy (-4.3 per 100 000 persons in males, -4.6 per 100 000 persons in females), appendectomy (-12.3 per 100 000 persons in males, -12.2 per 100 000 persons in females), and colorectal resection (-9.0 per 100 000 persons in males, -12.7 per 100 000 persons in females), the disparity remained constant for coronary artery bypass grafting and widened for 3 procedures, total hip arthroplasty (11.6 per 100 000 persons in males, 20.8 per 100 000 in females), total knee arthroplasty (19.9 per 100 000 persons in males, 12.0 per 100 000 persons in females), and heart valve replacement(12.4 per 100 000 persons in males, 9.2 per 100 000 persons in females). In 2017, racial differences persisted in all US census divisions and in both urban teaching and urban nonteaching hospitals. When rates were adjusted based on insurance status, Black patients with Medicare, Medicaid, and private insurance underwent lower rates of all procedures analyzed compared with White patients. For example, rate of spinal fusion in Black patients was 70.2% of the rate in White patients with Medicare, 56.5% to that of White patients with Medicaid, and 61.2% to that of White patients with private insurance.
Conclusions and relevance: Results of this study suggest that despite national initiatives, racial disparities have persisted for all analyzed procedures and worsened for one-third of the analyzed procedures. These disparities were evident regardless of US census division, hospital teaching status, or insurance status. Renewed initiatives to help diminish racial disparities and improve health care equality are warranted.
Conflict of interest statement
Figures
Comment in
-
Socioeconomic Factors, Urological Epidemiology and Practice Patterns.J Urol. 2021 Oct;206(4):1054-1056. doi: 10.1097/JU.0000000000002128. Epub 2021 Jul 20. J Urol. 2021. PMID: 34281349 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
