

Longitudinal Associations of Mental Disorders With Physical Diseases and Mortality Among 2.3 Million New Zealand Citizens
- PMID: 33439264
- PMCID: PMC7807295
- DOI: 10.1001/jamanetworkopen.2020.33448
Longitudinal Associations of Mental Disorders With Physical Diseases and Mortality Among 2.3 Million New Zealand Citizens
Abstract
Importance: Excess risk of physical disease and mortality has been observed among individuals with psychiatric conditions, suggesting that ameliorating mental disorders might also be associated with ameliorating the later onset of physical disability and early mortality. However, the temporal association between mental disorders and physical diseases remains unclear, as many studies have relied on retrospective recall, used cross-sectional designs or prospective designs with limited follow-up periods, or given inadequate consideration to preexisting physical illnesses.
Objective: To examine whether mental disorders are associated with subsequent physical diseases and mortality across 3 decades of observation.
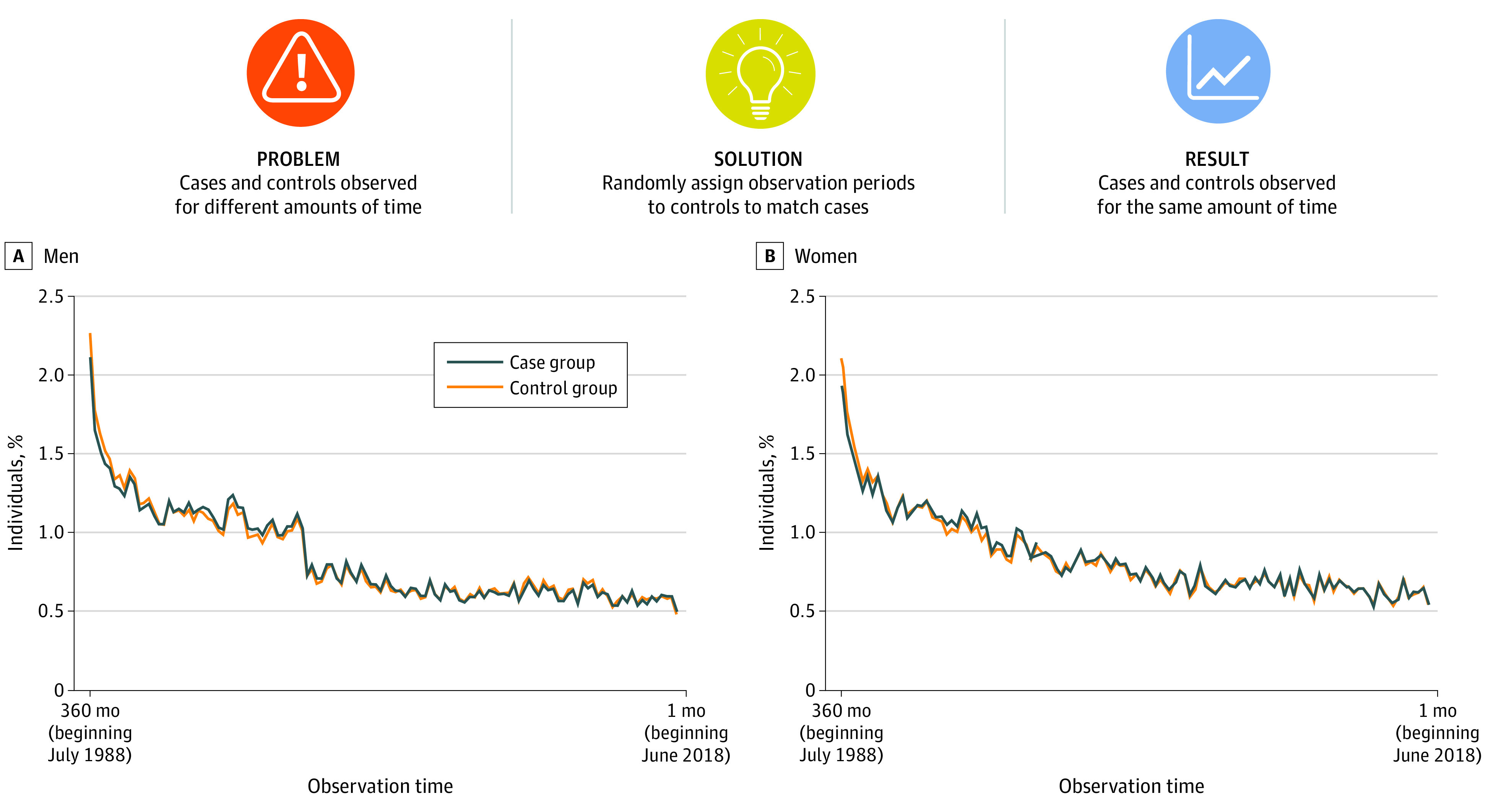
Design, setting, and participants: This population-based cohort study used data from the New Zealand Integrated Data Infrastructure, a collection of nationwide administrative data sources linked at the individual level, to identify mental disorders, physical diseases, and deaths recorded between July 1, 1988, and June 30, 2018, in the population of New Zealand. All individuals born in New Zealand between January 1, 1928, and December 31, 1978, who resided in the country at any time during the 30-year observation period were included in the analysis. Data were analyzed from July 2019 to November 2020.
Exposures: Nationwide administrative records of mental disorder diagnoses made in public hospitals.
Main outcomes and measures: Chronic physical disease diagnoses made in public hospitals, deaths, and health care use.
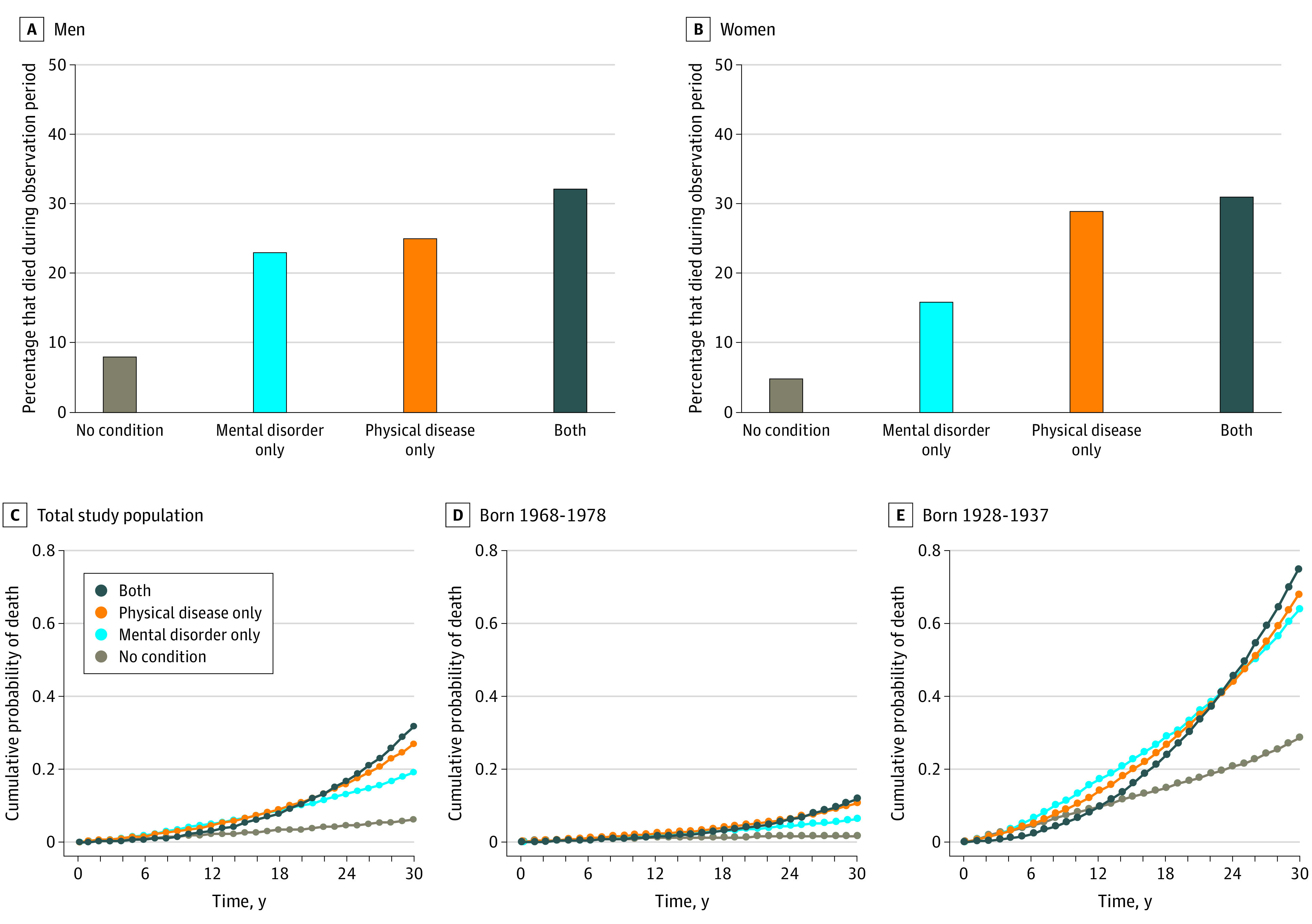
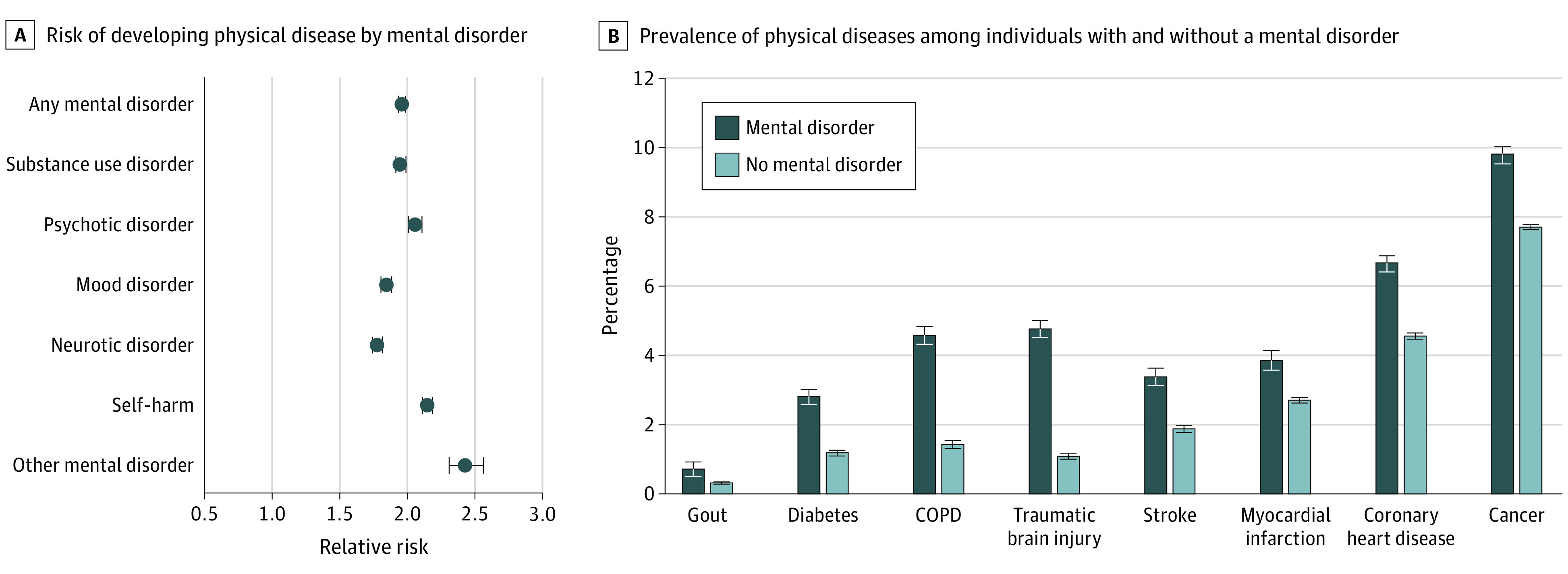
Results: The study population comprised 2 349 897 individuals (1 191 981 men [50.7%]; age range at baseline, 10-60 years). Individuals with a mental disorder developed subsequent physical diseases at younger ages (hazard ratio [HR], 2.33; 95% CI, 2.30-2.36) and died at younger ages (HR, 3.80; 95% CI, 3.72-3.89) than those without a mental disorder. These associations remained across sex and age and after accounting for preexisting physical diseases. Associations were observed across different types of mental disorders and self-harm behavior (relative risks, 1.78-2.43; P < .001 for all comparisons). Mental disorders were associated with the onset of physical diseases and the accumulation of physical disease diagnoses (incidence rate ratio [IRR], 2.00; 95% CI, 1.98-2.03), a higher number of hospitalizations (IRR, 2.43; 95% CI, 2.39-2.48), longer hospital stays for treatment (IRR, 2.70; 95% CI, 2.62-2.79), and higher associated health care costs (b = 0.115; 95% CI, 0.112-0.118).
Conclusions and relevance: In this study, mental disorders were likely to begin and peak in young adulthood, and they antedated physical diseases and early mortality in the population. These findings suggest that ameliorating mental disorders may have implications for improving the length and quality of life and for reducing the health care costs associated with physical diseases.
Conflict of interest statement
Figures

References
-
- LeVine S, Stevens H Deep dive: the aging, childless future. Axios. July 21, 2018. Accessed April 21, 2020. https://www.axios.com/the-aging-childless-future-21f9ae39-bf77-4777-8df2...
-
- World Economic Forum The Future of Jobs: Employment, Skills and Workforce Strategy for the Fourth Industrial Revolution World Economic Forum; 2016. Accessed June 25, 2020. http://www3.weforum.org/docs/WEF_Future_of_Jobs.pdf
-
- Cunningham R, Sarfati D, Peterson D, Stanley J, Collings S. Premature mortality in adults using New Zealand psychiatric services. N Z Med J. 2014;127(1394):31-41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
