

A template to quantify the location and density of CD3 + and CD8 + tumor-infiltrating lymphocytes in colon cancer by digital pathology on whole slides for an objective, standardized immune score assessment
- PMID: 33439293
- PMCID: PMC8195795
- DOI: 10.1007/s00262-020-02834-y
A template to quantify the location and density of CD3 + and CD8 + tumor-infiltrating lymphocytes in colon cancer by digital pathology on whole slides for an objective, standardized immune score assessment
Abstract
Background: In colon cancer, the location and density of tumor-infiltrating lymphocytes (TILs) can classify patients into low and high-risk groups for prognostication. While a commercially available 'Immunoscore®' exists, the incurred expenses and copyrights may prevent universal use. The aim of this study was to develop a robust and objective quantification method of TILs in colon cancer.
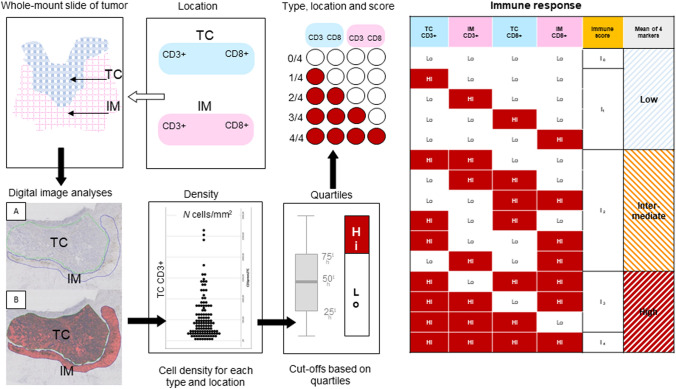
Methods: A consecutive, unselected series of specimens from patients with colon cancer were available for immunohistochemistry and assessment of TILs by automated digital pathology. CD3 + and CD8 + cells at the invasive margin and in tumor center were assessed on consecutive sections using automated digital pathology and image analysis software (Visiopharm®). An algorithm template for whole slide assessment, generated cell counts per square millimeters (cells/mm2), from which the immune score was calculated using distribution volumes. Furthermore, immune score was compared with clinical and histopathological characteristics to confirm its relevance.
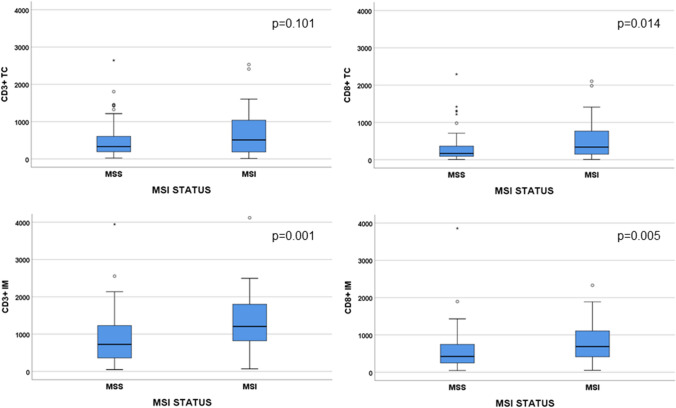
Results: Based on the quantified TILs numbers by digital image analyses, patients were classified into low (n = 83, 69.7%), intermediate (n = 14, 11.8%) and high (n = 22, 18.5%) immune score groups. High immune score was associated with stage I-II tumors (p = 0.017) and a higher prevalence of microsatellite instable (MSI) tumors (p = 0.030). MSI tumors had a significantly higher numbers of CD3 + TILs in the invasive margin and CD8 + TILs in both tumor center and invasive margin, compared to microsatellite stable (MSS) tumors.
Conclusion: A digital template to quantify an easy-to-use immune score corresponds with clinicopathological features and MSI in colon cancer.
Keywords: Colorectal cancer; Digital image analysis; Immune response; Tumor center; Tumor-infiltrating lymphocytes; Tumor-invasive margin.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Safiri S, Sepanlou SG, Ikuta KS, Bisignano C, Salimzadeh H, Delavari A, Ansari R, Roshandel G, Merat S, Fitzmaurice C, Force LM. The global, regional, and national burden of colorectal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2019;4(12):913–933. doi: 10.1016/s2468-1253(19)30345-0. - DOI - PMC - PubMed
-
- Lea D, Håland S, Hagland HR, Søreide K. Accuracy of TNM staging in colorectal cancer: a review of current culprits, the modern role of morphology and stepping-stones for improvements in the molecular era. Scand J Gastroenterol. 2014;49(10):1153–1163. doi: 10.3109/00365521.2014.950692. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
