

Prognostic Value of Abdominal Aortic Calcification: A Systematic Review and Meta-Analysis of Observational Studies
- PMID: 33439672
- PMCID: PMC7955302
- DOI: 10.1161/JAHA.120.017205
Prognostic Value of Abdominal Aortic Calcification: A Systematic Review and Meta-Analysis of Observational Studies
Abstract
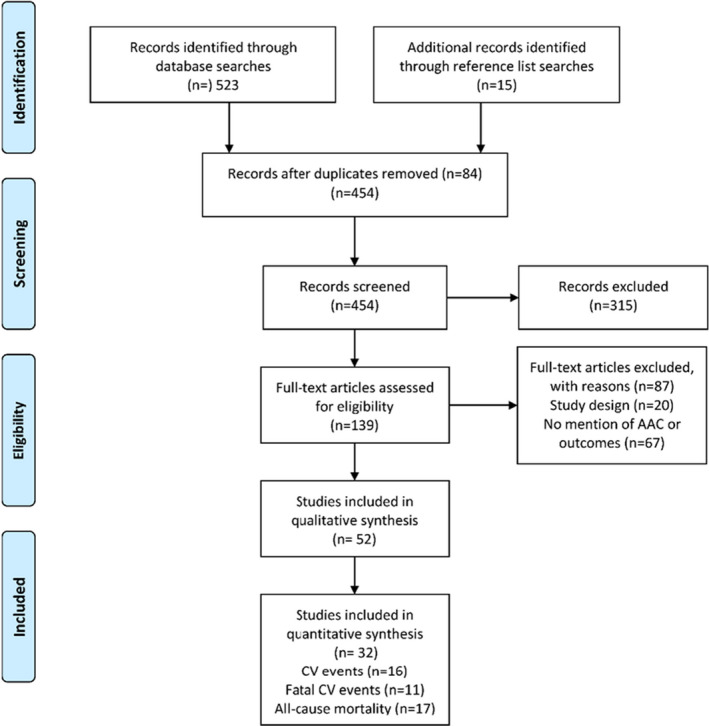
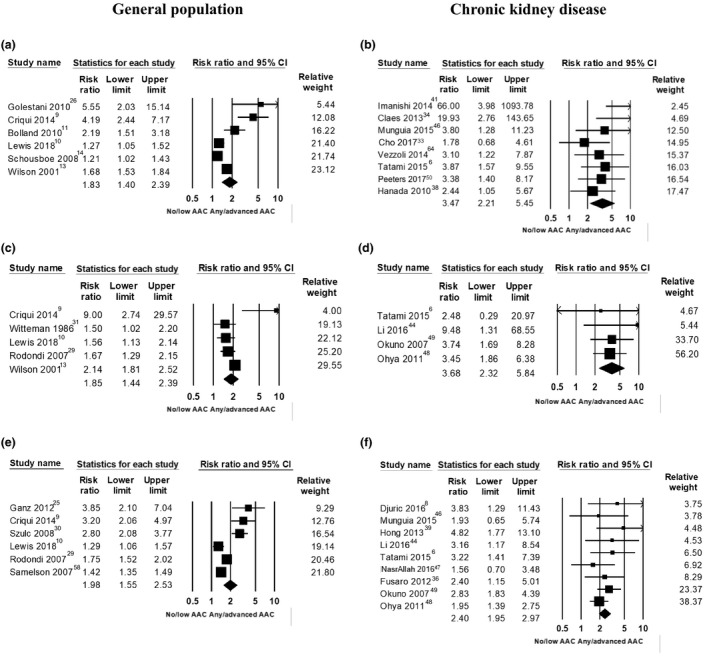
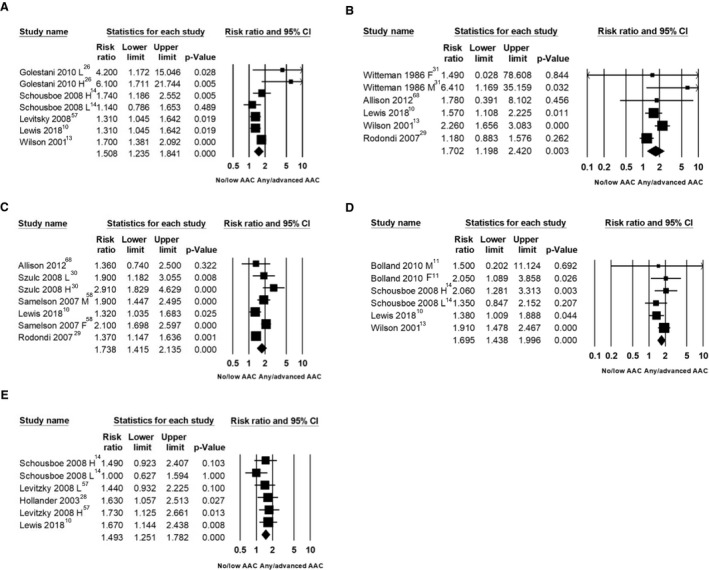
Background The prognostic importance of abdominal aortic calcification (AAC) viewed on noninvasive imaging modalities remains uncertain. Methods and Results We searched electronic databases (MEDLINE and Embase) until March 2018. Multiple reviewers identified prospective studies reporting AAC and incident cardiovascular events or all-cause mortality. Two independent reviewers assessed eligibility and risk of bias and extracted data. Summary risk ratios (RRs) were estimated using random-effects models comparing the higher AAC groups combined (any or more advanced AAC) to the lowest reported AAC group. We identified 52 studies (46 cohorts, 36 092 participants); only studies of patients with chronic kidney disease (57%) and the general older-elderly (median, 68 years; range, 60-80 years) populations (26%) had sufficient data to meta-analyze. People with any or more advanced AAC had higher risk of cardiovascular events (RR, 1.83; 95% CI, 1.40-2.39), fatal cardiovascular events (RR, 1.85; 95% CI, 1.44-2.39), and all-cause mortality (RR, 1.98; 95% CI, 1.55-2.53). Patients with chronic kidney disease with any or more advanced AAC had a higher risk of cardiovascular events (RR, 3.47; 95% CI, 2.21-5.45), fatal cardiovascular events (RR, 3.68; 95% CI, 2.32-5.84), and all-cause mortality (RR, 2.40; 95% CI, 1.95-2.97). Conclusions Higher-risk populations, such as the elderly and those with chronic kidney disease with AAC have substantially greater risk of future cardiovascular events and poorer prognosis. Providing information on AAC may help clinicians understand and manage patients' cardiovascular risk better.
Keywords: abdominal aortic calcification; all‐cause mortality; cardiovascular events and deaths; chronic kidney disease; general population.
Conflict of interest statement
None.
Figures

Similar articles
-
Abdominal aortic calcification can predict all-cause mortality and CV events in dialysis patients: A systematic review and meta-analysis.PLoS One. 2018 Sep 21;13(9):e0204526. doi: 10.1371/journal.pone.0204526. eCollection 2018. PLoS One. 2018. PMID: 30240443 Free PMC article.
-
Abdominal aortic calcification, bone mineral density and fractures: a systematic review and meta-analysis protocol.BMJ Open. 2019 Apr 2;9(4):e026232. doi: 10.1136/bmjopen-2018-026232. BMJ Open. 2019. PMID: 30944137 Free PMC article.
-
Abdominal aorta calcification predicts cardiovascular but not non-cardiovascular outcome in patients receiving peritoneal dialysis: A prospective cohort study.Medicine (Baltimore). 2020 Sep 11;99(37):e21730. doi: 10.1097/MD.0000000000021730. Medicine (Baltimore). 2020. PMID: 32925715 Free PMC article.
-
Impact of abdominal aortic calcification on long-term cardiovascular outcomes in patients with chronic kidney disease.Atherosclerosis. 2015 Dec;243(2):349-55. doi: 10.1016/j.atherosclerosis.2015.10.016. Epub 2015 Oct 22. Atherosclerosis. 2015. PMID: 26519631
-
Calcification of the abdominal aorta as an independent predictor of cardiovascular events: a meta-analysis.Heart. 2012 Jul;98(13):988-94. doi: 10.1136/heartjnl-2011-301464. Heart. 2012. PMID: 22668866 Review.
Cited by
-
Phenotypic plasticity of vascular smooth muscle cells in vascular calcification: Role of mitochondria.Front Cardiovasc Med. 2022 Oct 12;9:972836. doi: 10.3389/fcvm.2022.972836. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312244 Free PMC article. Review.
-
A Novel Quantitative Computer-Assisted Score Can Improve Repeatability in the Estimate of Vascular Calcifications at the Abdominal Aorta.Nutrients. 2022 Oct 13;14(20):4276. doi: 10.3390/nu14204276. Nutrients. 2022. PMID: 36296959 Free PMC article.
-
DXA beyond bone mineral density and the REMS technique: new insights for current radiologists practice.Radiol Med. 2024 Aug;129(8):1224-1240. doi: 10.1007/s11547-024-01843-6. Epub 2024 Jul 30. Radiol Med. 2024. PMID: 39080226 Free PMC article. Review.
-
Association between hemoglobin A1c and abdominal aortic calcification: results from the National Health and Nutrition Examination Survey 2013-2014.BMC Cardiovasc Disord. 2024 Jan 3;24(1):26. doi: 10.1186/s12872-023-03700-2. BMC Cardiovasc Disord. 2024. PMID: 38172671 Free PMC article.
-
The estimated glomerular filtration rate was U-shaped associated with abdominal aortic calcification in US adults: findings from NHANES 2013-2014.Front Cardiovasc Med. 2023 Dec 6;10:1261021. doi: 10.3389/fcvm.2023.1261021. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 38124889 Free PMC article.
References
-
- Budoff MJ, Shaw LJ, Liu ST, Weinstein SR, Mosler TP, Tseng PH, Flores FR, Callister TQ, Raggi P, Berman DS. Long‐term prognosis associated with coronary calcification: observations from a registry of 25,253 patients. J Am Coll Cardiol. 2007;49:1860–1870. - PubMed
-
- Szulc P. Abdominal aortic calcification: a reappraisal of epidemiological and pathophysiological data. Bone. 2016;84:25–37. - PubMed
-
- Strong JP, Malcom GT, McMahan CA, Tracy RE, Newman WP III, Herderick EE, Cornhill JF. Prevalence and extent of atherosclerosis in adolescents and young adults: implications for prevention from the pathobiological determinants of atherosclerosis in youth study. JAMA. 1999;281:727–735. - PubMed
-
- Allam AHA, Thompson RC, Eskander MA, Mandour Ali MA, Sadek A, Rowan CJ, Sutherland ML, Sutherland JD, Frohlich B, Michalik DE, et al. Is coronary calcium scoring too late? Total body arterial calcium burden in patients without known CAD and normal MPI. J Nucl Cardiol. 2018;25:1990–1998. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
