

Sex differences in susceptibility, severity, and outcomes of coronavirus disease 2019: Cross-sectional analysis from a diverse US metropolitan area
- PMID: 33439908
- PMCID: PMC7806140
- DOI: 10.1371/journal.pone.0245556
Sex differences in susceptibility, severity, and outcomes of coronavirus disease 2019: Cross-sectional analysis from a diverse US metropolitan area
Abstract
Introduction: Sex is increasingly recognized as an important factor in the epidemiology and outcome of many diseases. This also appears to hold for coronavirus disease 2019 (COVID-19). Evidence from China and Europe has suggested that mortality from COVID-19 infection is higher in men than women, but evidence from US populations is lacking. Utilizing data from a large healthcare provider, we determined if males, as compared to females have a higher likelihood of SARS-CoV-2 susceptibility, and if among the hospitalized COVID-19 patients, male sex is independently associated with COVID-19 severity and poor in-hospital outcomes.
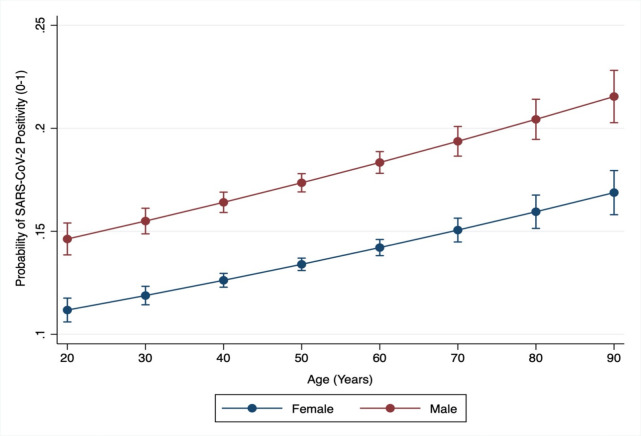
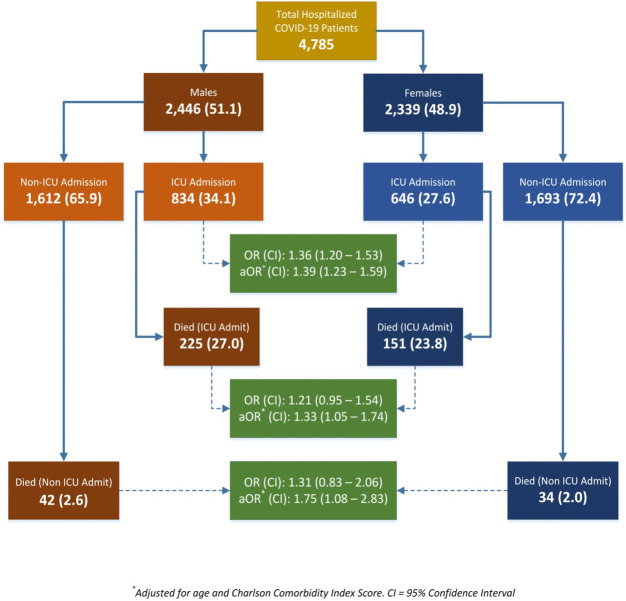
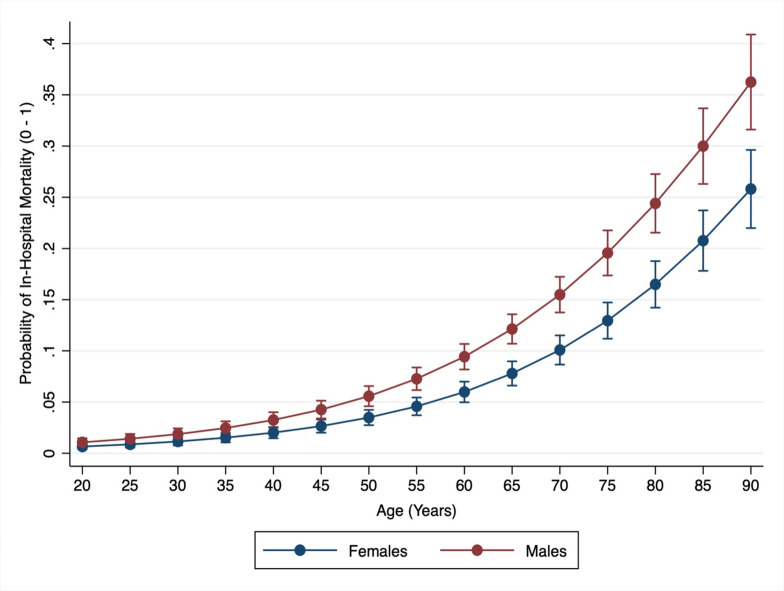
Methods and findings: Using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, we conducted a cross-sectional analysis of data from a COVID-19 Surveillance and Outcomes Registry (CURATOR). Data were extracted from Electronic Medical Records (EMR). A total of 96,473 individuals tested for SARS-CoV-2 RNA in nasopharyngeal swab specimens via Polymerized Chain Reaction (PCR) tests were included. For hospital-based analyses, all patients admitted during the same time-period were included. Of the 96,473 patients tested, 14,992 (15.6%) tested positive, of whom 4,785 (31.9%) were hospitalized and 452 (9.5%) died. Among all patients tested, men were significantly older. The overall SARS-CoV-2 positivity among all tested individuals was 15.5%, and was higher in males as compared to females 17.0% vs. 14.6% [OR 1.20]. This sex difference held after adjusting for age, race, ethnicity, marital status, insurance type, median income, BMI, smoking and 17 comorbidities included in Charlson Comorbidity Index (CCI) [aOR 1.39]. A higher proportion of males (vs. females) experienced pulmonary (ARDS, hypoxic respiratory failure) and extra-pulmonary (acute renal injury) complications during their hospital course. After adjustment, length of stay (LOS), need for mechanical ventilation, and in-hospital mortality were significantly higher in males as compared to females.
Conclusions: In this analysis of a large US cohort, males were more likely to test positive for COVID-19. In hospitalized patients, males were more likely to have complications, require ICU admission and mechanical ventilation, and had higher mortality than females, independent of age. Sex disparities in COVID-19 vulnerability are present, and emphasize the importance of examining sex-disaggregated data to improve our understanding of the biological processes involved to potentially tailor treatment and risk stratify patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Razzaghi H, Wang Y, Lu H, Marshall KE, Dowling NF, Paz-Bailey G, et al. Estimated County-Level Prevalence of Selected Underlying Medical Conditions Associated with Increased Risk for Severe COVID-19 Illness—United States, 2018. MMWR Morb Mortal Wkly Rep 2020;69:945–50. 10.15585/mmwr.mm6929a1 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
