

The benefits and costs of social distancing in high- and low-income countries
- PMID: 33440007
- PMCID: PMC7928561
- DOI: 10.1093/trstmh/traa140
The benefits and costs of social distancing in high- and low-income countries
Abstract
Background: Widespread social distancing and lockdowns of everyday activity have been the primary policy prescription across many countries throughout the coronavirus disease 2019 (COVID-19) pandemic. Despite their uniformity, these measures may be differentially valuable for different countries.
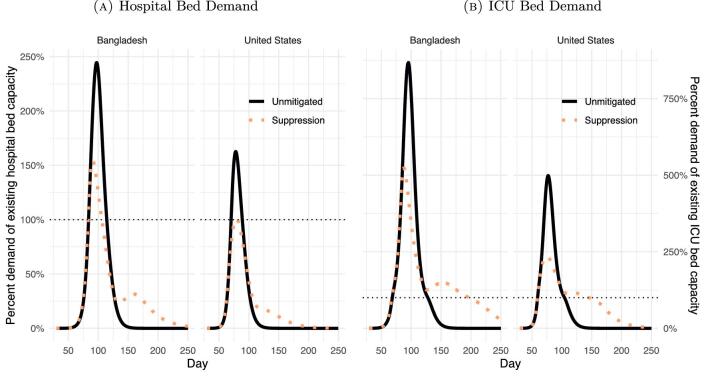
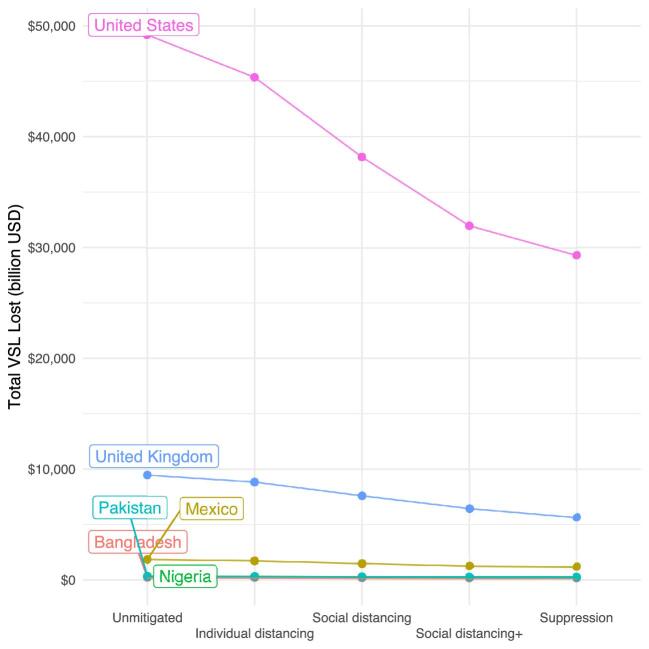
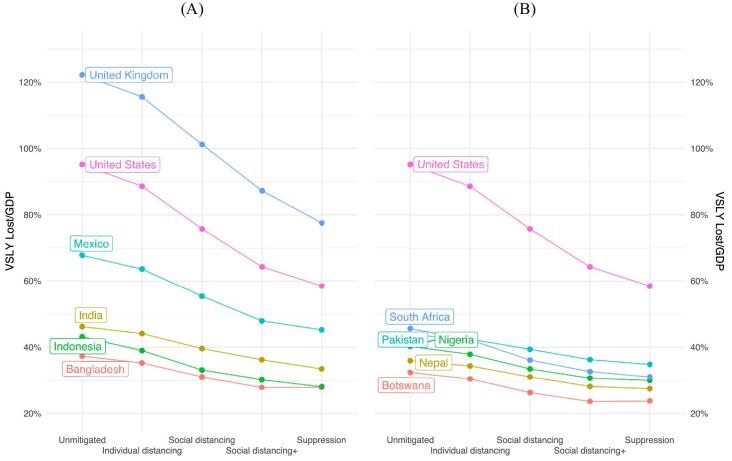
Methods: We use a compartmental epidemiological model to project the spread of COVID-19 across policy scenarios in high- and low-income countries. We embed estimates of the welfare value of disease avoidance into the epidemiological projections to estimate the return to more stringent lockdown policies.
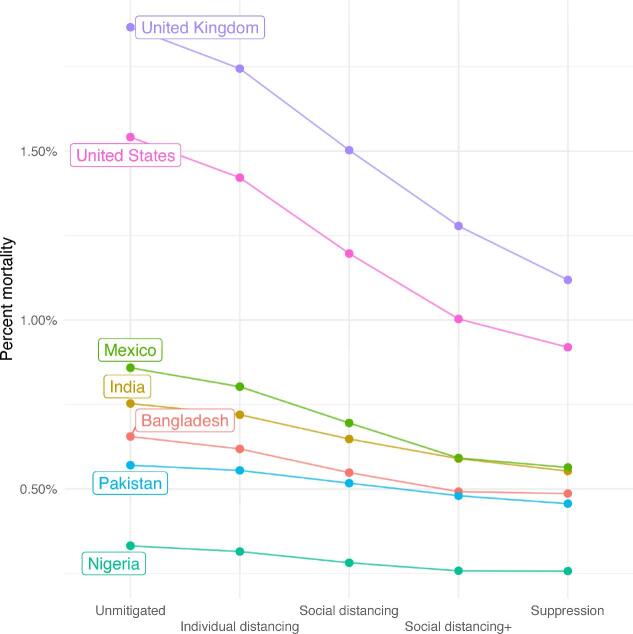
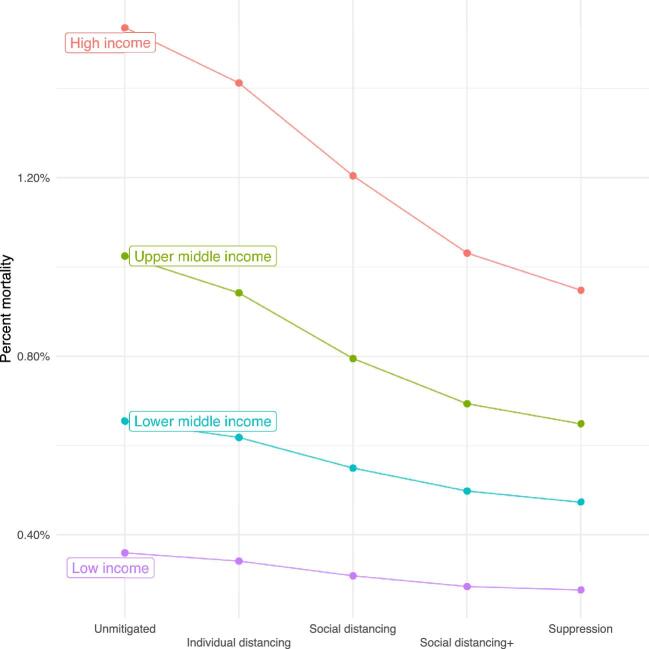
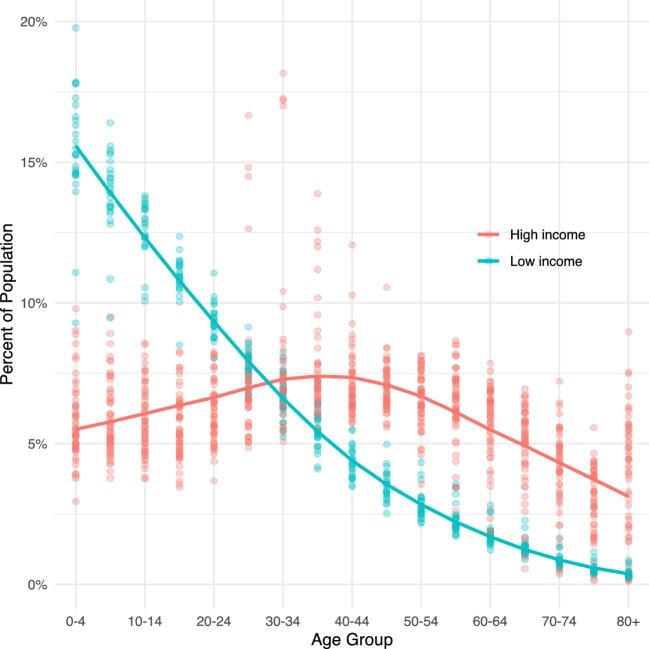
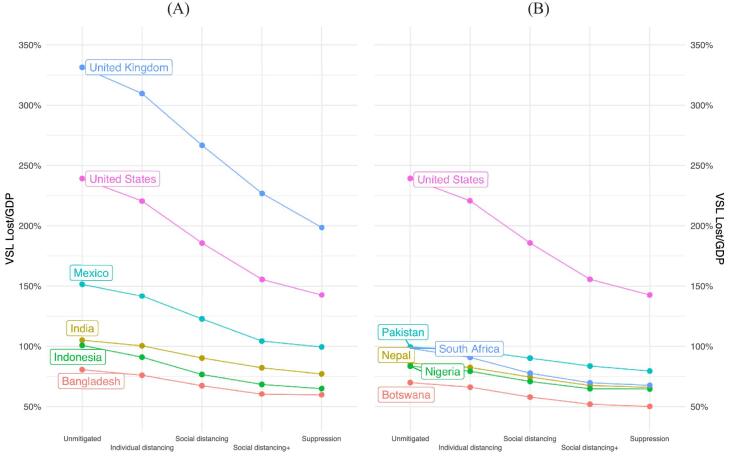
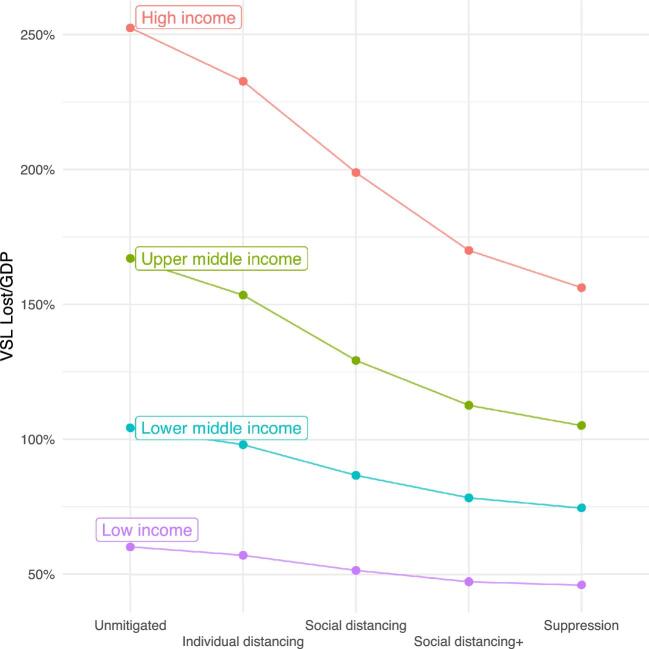
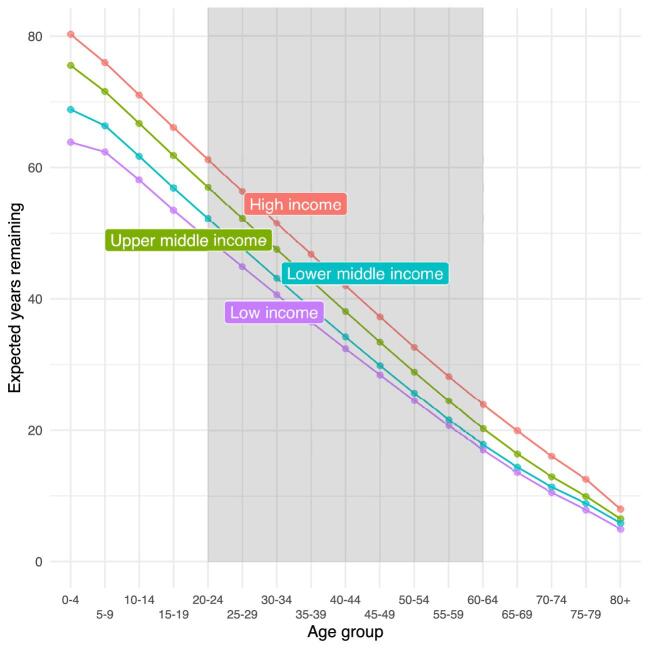
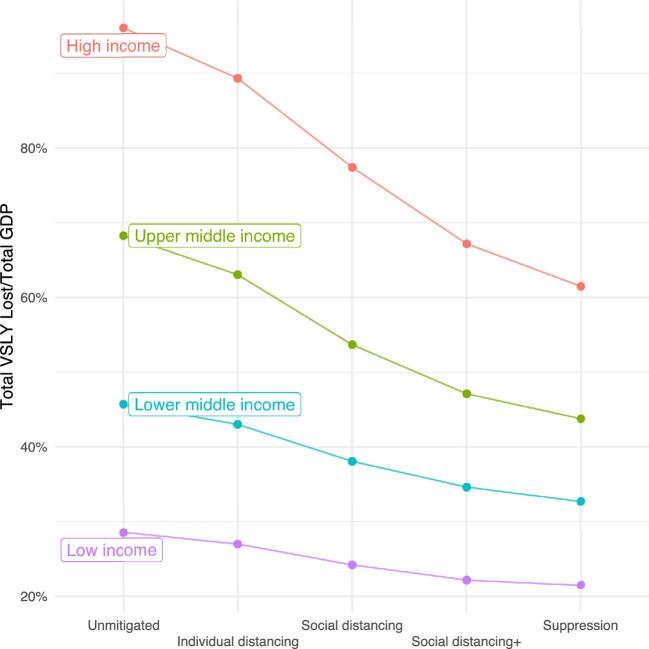
Results: Social distancing measures that 'flatten the curve' of the disease provide immense welfare value in upper-income countries. However, social distancing policies deliver significantly less value in lower-income countries that have younger populations, which are less vulnerable to COVID-19. Equally important, social distancing mandates a trade-off between disease risk and economic activity. Poorer people are less able to make those economic sacrifices.
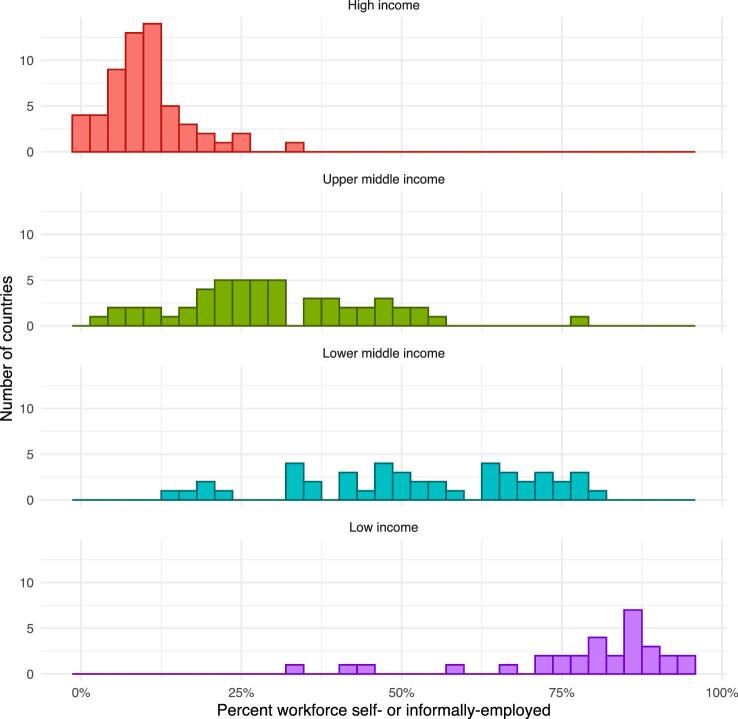
Conclusions: The epidemiological and welfare value of social distancing is smaller in lower-income countries and such policies may exact a heavy toll on the poorest and most vulnerable. Workers in the informal sector often lack the resources and social protections that enable them to isolate themselves until the virus passes. By limiting these households' ability to earn a living, social distancing can lead to an increase in hunger, deprivation, and related mortality and morbidity.
Keywords: COVID-19; VSL; global health; pandemics; social distancing; welfare economics.
© The Author(s) 2021. Published by Oxford University Press on behalf of Royal Society of Tropical Medicine and Hygiene.
Figures
References
-
- Watson OJ, Walker P, Whittaker C et al. squire version 0.4.34. Available from: https://mrc-ide.github.io/squire/index.html (accessed 17 December 2020).
-
- COVID-19 community mobility reports. Available from: https://www.google.com/covid19/mobility/ (accessed 17 December 2020).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
