

Pretomanid dose selection for pulmonary tuberculosis: An application of multi-objective optimization to dosage regimen design
- PMID: 33440076
- PMCID: PMC7965837
- DOI: 10.1002/psp4.12591
Pretomanid dose selection for pulmonary tuberculosis: An application of multi-objective optimization to dosage regimen design
Abstract
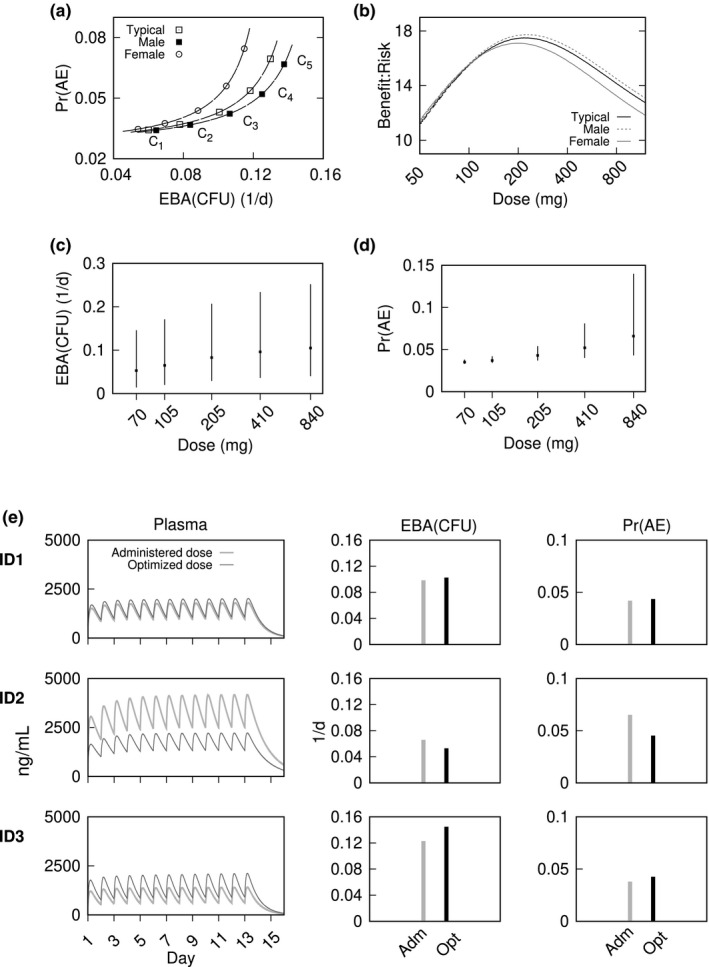
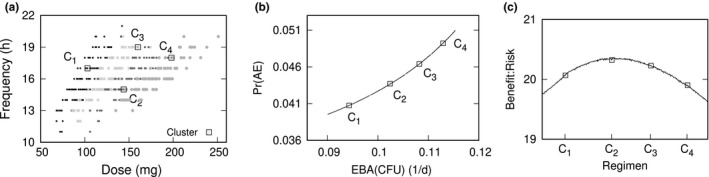
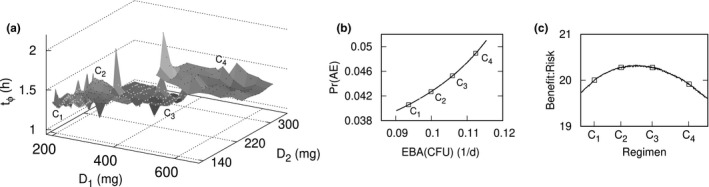
Clinical development of combination chemotherapies for tuberculosis (TB) is complicated by partial or restricted phase II dose-finding. Barriers include a propensity for drug resistance with monotherapy, practical limits on numbers of treatment arms for component dose combinations, and limited application of current dose selection methods to multidrug regimens. A multi-objective optimization approach to dose selection was developed as a conceptual and computational framework for currently evolving approaches to clinical testing of novel TB regimens. Pharmacokinetic-pharmacodynamic (PK-PD) modeling was combined with an evolutionary algorithm to identify dosage regimens that yield optimal trade-offs between multiple conflicting therapeutic objectives. The phase IIa studies for pretomanid, a newly approved nitroimidazole for specific cases of highly drug-resistant pulmonary TB, were used to demonstrate the approach with Pareto optimized dosing that best minimized sputum bacillary load and the probability of drug-related adverse events. Results include a population-typical characterization of the recommended 200 mg once daily dosage, the optimality of time-dependent dosing, examples of individualized therapy, and the determination of optimal loading doses. The approach generalizes conventional PK-PD target attainment to a design problem that scales to drug combinations, and provides a benefit-risk context for clinical testing of complex drug regimens.
© 2021 The Author. CPT: Pharmacometrics & Systems Pharmacology published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The author declared no competing interests for this work.
Figures
References
-
- World Health Organization . Global Tuberculosis Report 2019. Geneva: World Health Organization; 2019. License: CCBY‐NC‐SA3.0IGO.
-
- Murray S, Mendel C, Spigelman M. TB Alliance regimen development for multidrug‐resistant tuberculosis. Int J Tuberc Lung Dis. 2016;20:S38–S41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
