

Long-Term Survival of Patients With Left Ventricular Noncompaction
- PMID: 33441029
- PMCID: PMC7955291
- DOI: 10.1161/JAHA.119.015563
Long-Term Survival of Patients With Left Ventricular Noncompaction
Abstract
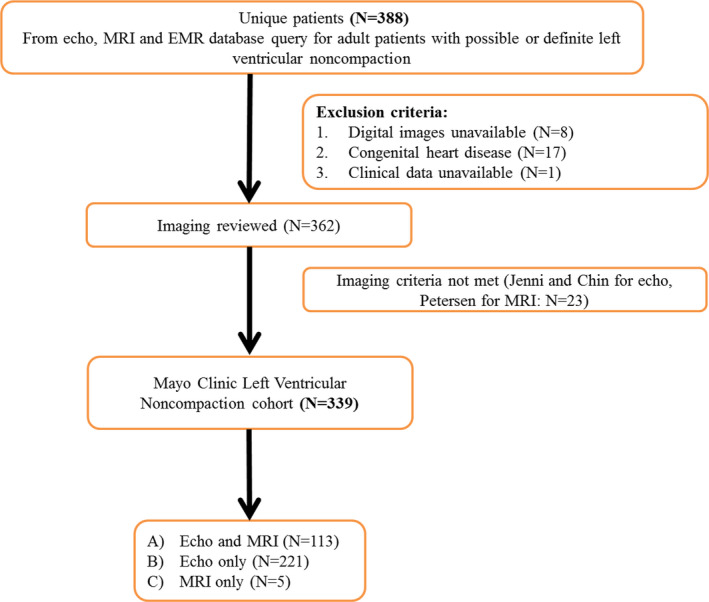
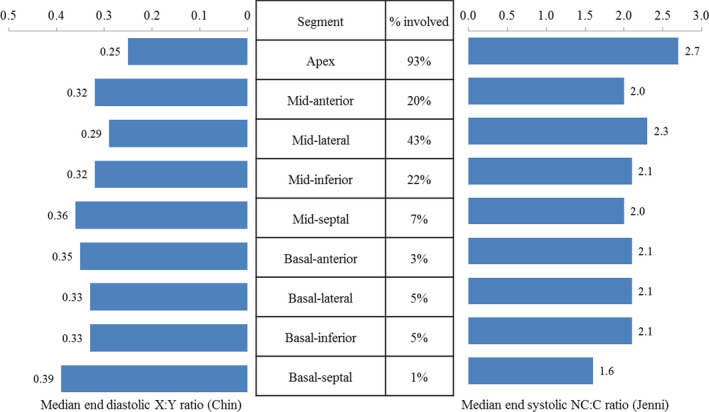
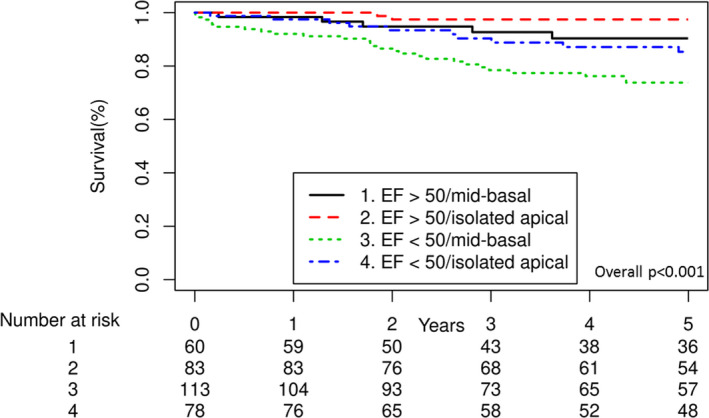
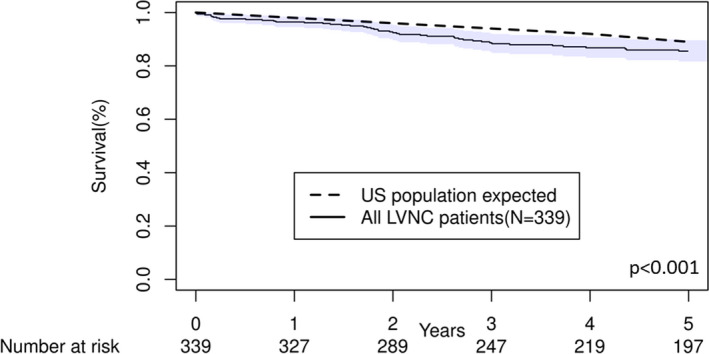
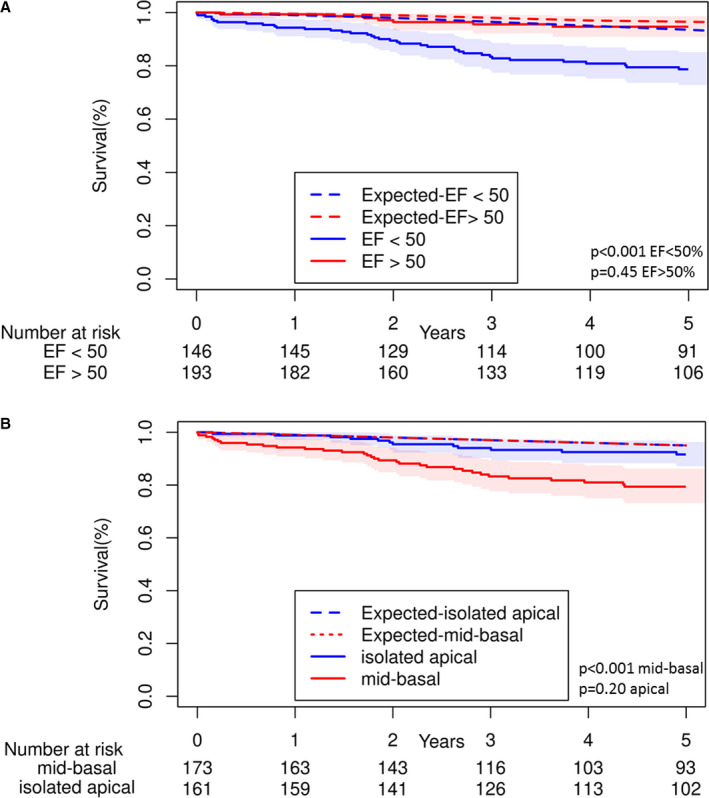
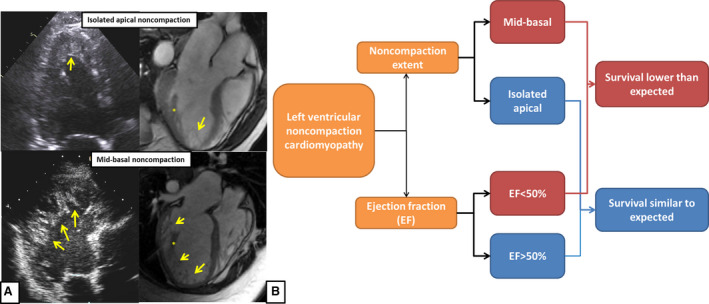
Background The prognosis of left ventricular noncompaction (LVNC) remains elusive despite its recognition as a clinical entity for >30 years. We sought to identify clinical and imaging characteristics and risk factors for mortality in patients with LVNC. Methods and Results 339 adults with LVNC seen between 2000 and 2016 were identified. LVNC was defined as end-systolic noncompacted to compacted myocardial ratio >2 (Jenni criteria) and end-diastolic trough of trabeculation-to-epicardium (X):peak of trabeculation-to-epicardium (Y) ratio <0.5 (Chin criteria) by echocardiography; and end-diastolic noncompacted:compacted ratio >2.3 (Petersen criteria) by magnetic resonance imaging. Median age was 47.4 years, and 46% of patients were female. Left ventricular ejection fraction <50% was present in 57% of patients and isolated apical noncompaction in 48%. During a median follow-up of 6.3 years, 59 patients died. On multivariable Cox regression analysis, age (hazard ratio [HR] 1.04; 95% CI, 1.02-1.06), left ventricular ejection fraction <50% (HR, 2.37; 95% CI, 1.17-4.80), and noncompaction extending from the apex to the mid or basal segments (HR, 2.11; 95% CI, 1.21-3.68) were associated with all-cause mortality. Compared with the expected survival for age- and sex-matched US population, patients with LVNC had reduced overall survival (P<0.001). However, patients with LVNC with preserved left ventricular ejection fraction and patients with isolated apical noncompaction had similar survival to the general population. Conclusions Overall survival is reduced in patients with LVNC compared with the expected survival of age- and sex-matched US population. However, survival rate in those with preserved left ventricular ejection fraction and isolated apical noncompaction was comparable with that of the general population.
Keywords: ejection fraction; mortality; noncompaction; prognosis; survival.
Conflict of interest statement
None.
Figures
Comment in
-
Left Ventricular Noncompaction Cardiomyopathy: New Clues in a Not So New Disease?J Am Heart Assoc. 2021 Jan 19;10(2):e018815. doi: 10.1161/JAHA.120.018815. Epub 2021 Jan 14. J Am Heart Assoc. 2021. PMID: 33442993 Free PMC article. No abstract available.
References
-
- Towbin JA, Lorts A, Jefferies JL. Left ventricular non‐compaction cardiomyopathy. Lancet. 2015;386:813–825. - PubMed
-
- Chin TK, Perloff JK, Williams RG, Jue K, Mohrmann R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation. 1990;82:507–513. - PubMed
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, Dubourg O, Kuhl U, Maisch B, McKenna WJ, et al. Classification of the cardiomyopathies: a position statement from the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270–276. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
