

Disease severity-specific neutrophil signatures in blood transcriptomes stratify COVID-19 patients
- PMID: 33441124
- PMCID: PMC7805430
- DOI: 10.1186/s13073-020-00823-5
Disease severity-specific neutrophil signatures in blood transcriptomes stratify COVID-19 patients
Abstract
Background: The SARS-CoV-2 pandemic is currently leading to increasing numbers of COVID-19 patients all over the world. Clinical presentations range from asymptomatic, mild respiratory tract infection, to severe cases with acute respiratory distress syndrome, respiratory failure, and death. Reports on a dysregulated immune system in the severe cases call for a better characterization and understanding of the changes in the immune system.
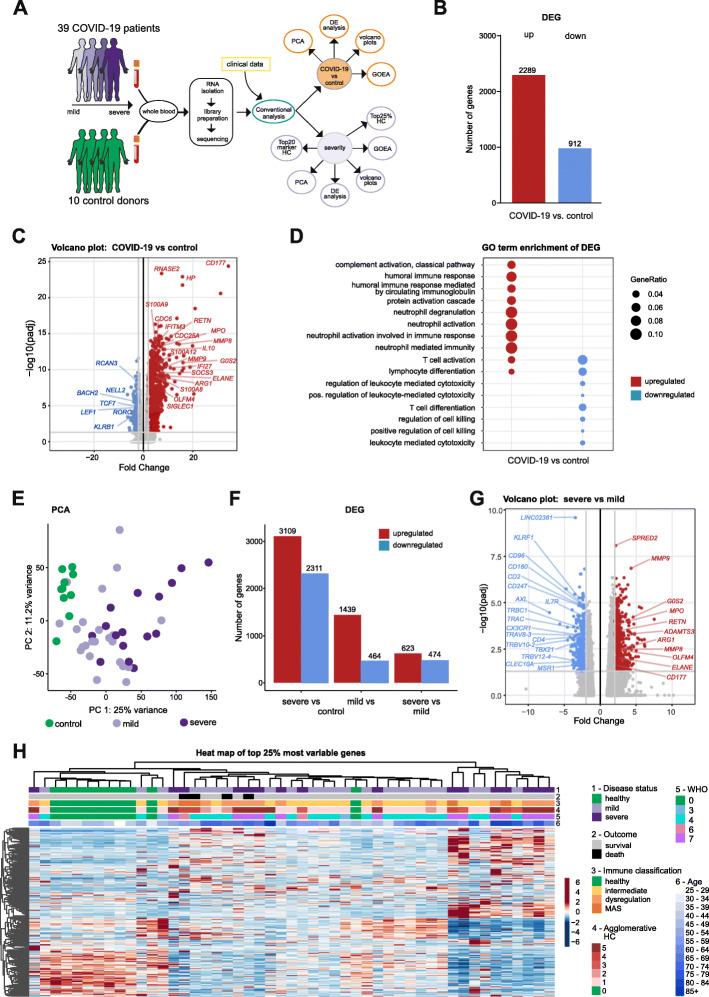
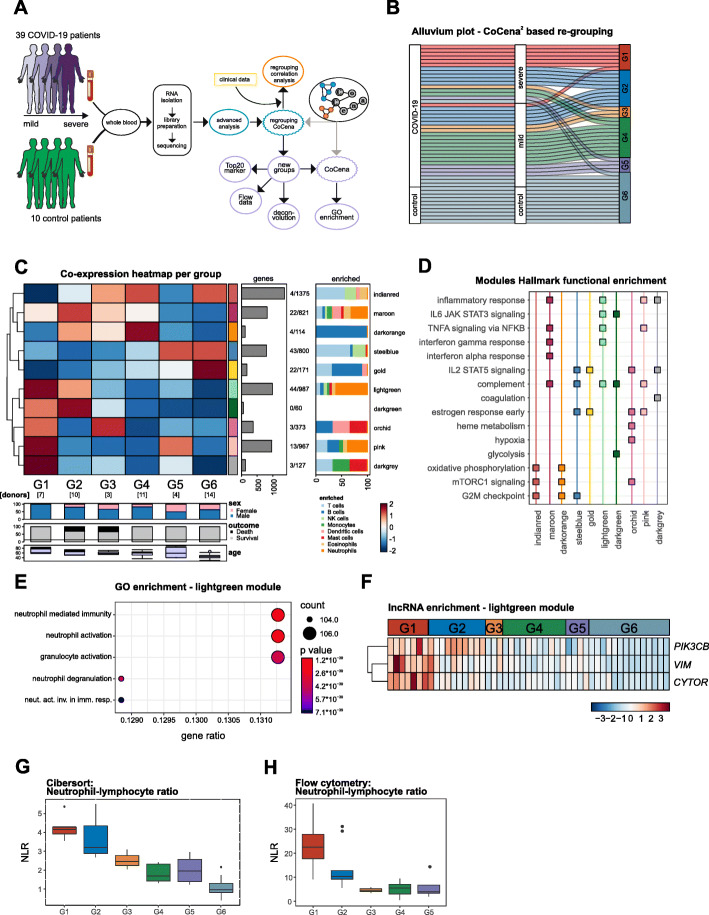
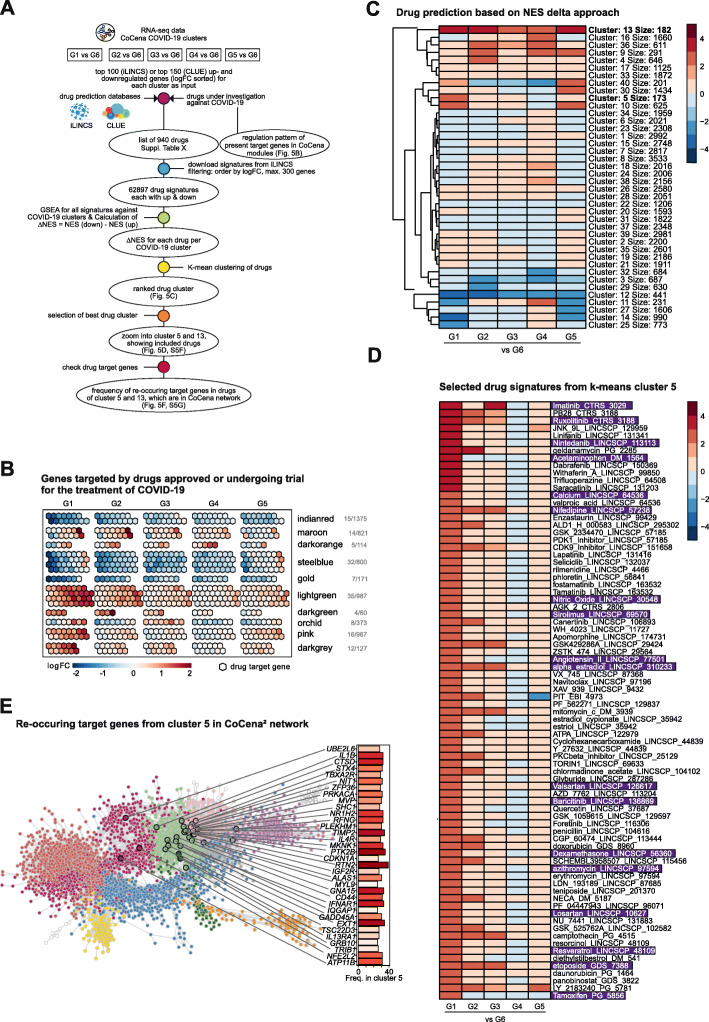
Methods: In order to dissect COVID-19-driven immune host responses, we performed RNA-seq of whole blood cell transcriptomes and granulocyte preparations from mild and severe COVID-19 patients and analyzed the data using a combination of conventional and data-driven co-expression analysis. Additionally, publicly available data was used to show the distinction from COVID-19 to other diseases. Reverse drug target prediction was used to identify known or novel drug candidates based on finding from data-driven findings.
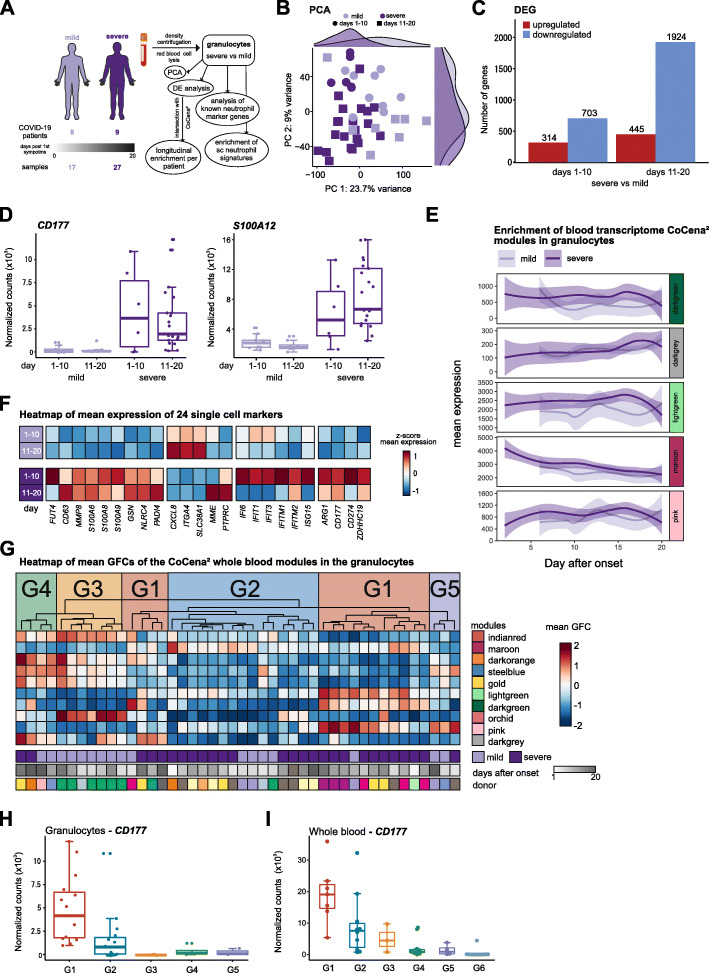
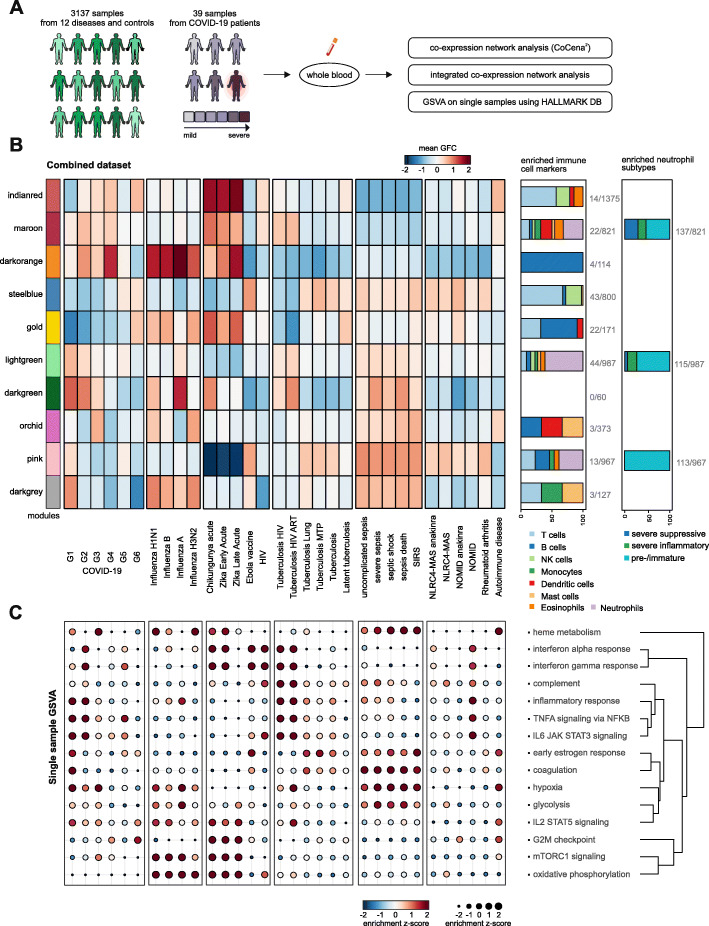
Results: Here, we profiled whole blood transcriptomes of 39 COVID-19 patients and 10 control donors enabling a data-driven stratification based on molecular phenotype. Neutrophil activation-associated signatures were prominently enriched in severe patient groups, which was corroborated in whole blood transcriptomes from an independent second cohort of 30 as well as in granulocyte samples from a third cohort of 16 COVID-19 patients (44 samples). Comparison of COVID-19 blood transcriptomes with those of a collection of over 3100 samples derived from 12 different viral infections, inflammatory diseases, and independent control samples revealed highly specific transcriptome signatures for COVID-19. Further, stratified transcriptomes predicted patient subgroup-specific drug candidates targeting the dysregulated systemic immune response of the host.
Conclusions: Our study provides novel insights in the distinct molecular subgroups or phenotypes that are not simply explained by clinical parameters. We show that whole blood transcriptomes are extremely informative for COVID-19 since they capture granulocytes which are major drivers of disease severity.
Keywords: Blood transcriptomics; COVID-19; Co-expression analysis; Drug repurposing; Granulocytes; Molecular disease phenotypes; Neutrophils; Stratification; Transcriptome.
Conflict of interest statement
EJG-B has received honoraria (paid to the University of Athens) from AbbVie USA, Abbott CH, Angelini Italy, Biotest Germany, InflaRx GmbH, MSD Greece, and XBiotech Inc. He has received independent educational grants from AbbVie, Abbott, Astellas Pharma, AxisShield, bioMérieux Inc., InflaRx GmbH, and XBiotech Inc.
The remaining authors declare that they have no competing interests.
Figures
References
-
- Brignola C, Campieri M, Farruggia P, Tragnone A, Pasquali S, Iannone P, et al. The possible utility of steroids in the prevention of relapses of Crohn’s disease in remission: a preliminary study. J Clin Gastroenterol. 1988;10(6):631–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
