

Purely laparoscopic feeding jejunostomy: a procedure which deserves more attention
- PMID: 33441134
- PMCID: PMC7805100
- DOI: 10.1186/s12893-021-01050-4
Purely laparoscopic feeding jejunostomy: a procedure which deserves more attention
Abstract
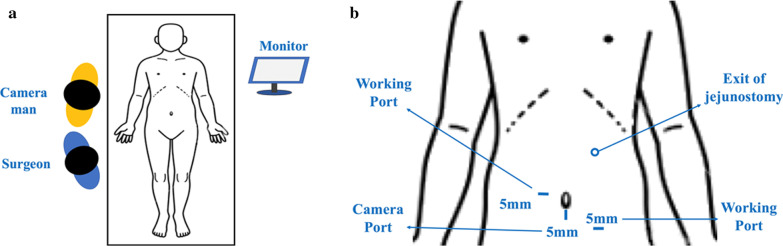
Background: Laparoscopic procedure has inherent merits of smaller incisions, better cosmesis, less postoperative pain, and earlier recovery. In the current study, we presented our method of purely laparoscopic feeding jejunostomy and compared its results with that of conventional open approach.
Methods: We retrospectively reviewed our patients from 2012 to 2019 who had received either laparoscopic jejunostomy (LJ, n = 29) or open ones (OJ, n = 94) in Chang Gung Memorial Hospital, Linkou. Peri-operative data and postoperative outcomes were analyzed.
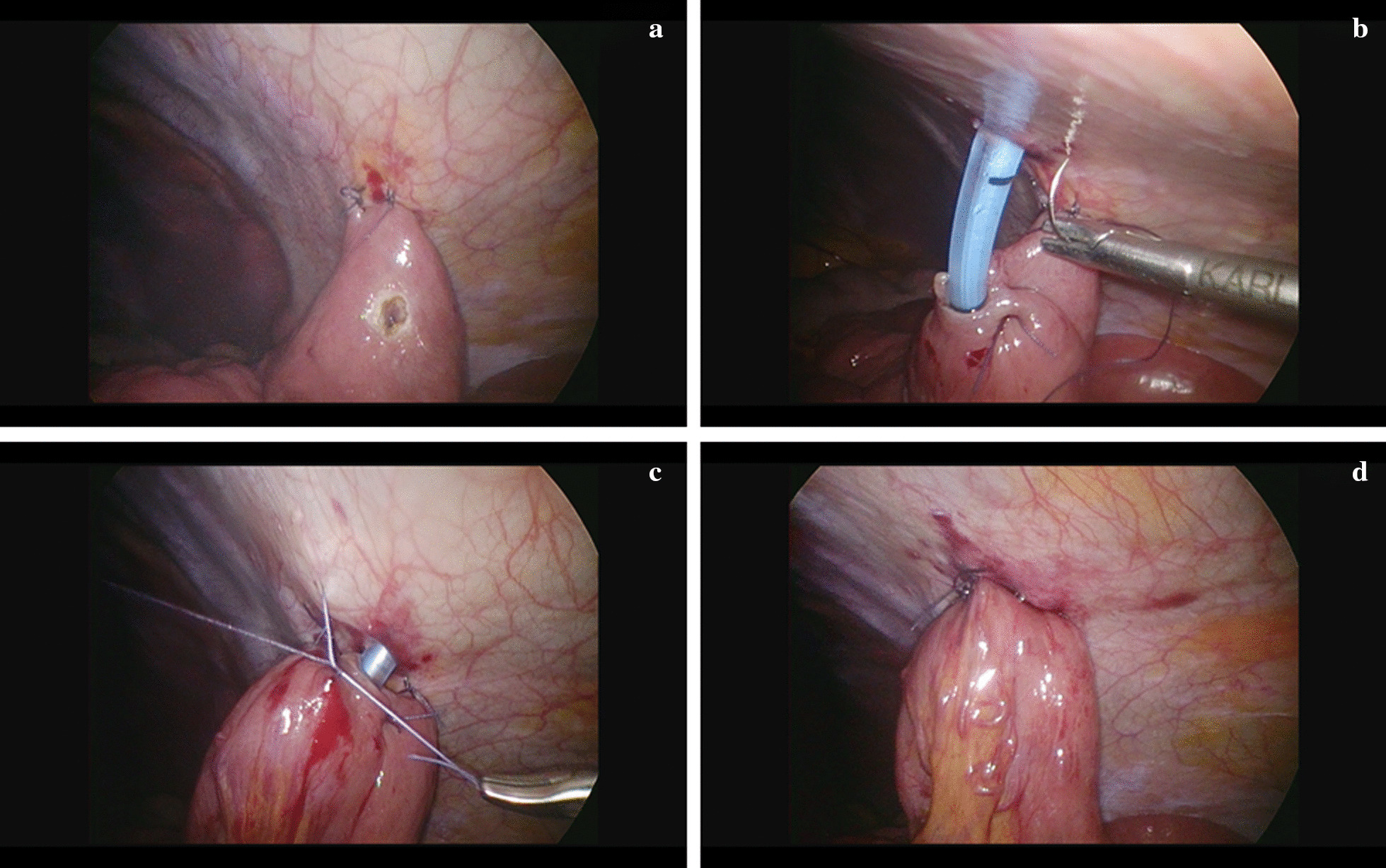
Results: In the current study, we employed 3-0 Vicryl, instead of V-loc barbed sutures, for laparoscopic jejunostomy. The mean operative duration of LJ group was about 30 min longer than the OJ group (159 ± 57.2 mins vs 128 ± 34.6 mins; P = 0.001). There were no intraoperative complications reported in both groups. The patients in the LJ group suffered significantly less postoperative pain than in the OJ group (mean NRS 2.03 ± 0.9 vs. 2.79 ± 1.2; P = 0.002). The majority of patients in both groups received early enteral nutrition (< 48 h) after the operation (86.2% vs. 74.5%; P = 0.143).
Conclusions: Our study demonstrated that purely laparoscopic feeding jejunostomy is a safe and feasible procedure with less postoperative pain and excellent postoperative outcome. It also provides surgeons opportunities to enhance intracorporeal suture techniques.
Keywords: Enteral nutrition; Enterostomy; Feeding; Jejunostomy; Minimally invasive surgery; Purely laparoscopic.
Conflict of interest statement
Hsin-I Tsai, Ta-Chun Chou, Ming-Chin Yu, Chun-Nan Yeh, Meng-Ting Peng, Chia-Hsun Hsieh, Po-Jung Su, Chiao-En Wu, Yung-Chia Kuo, Chien-Chih Chiu, and Chao-Wei Lee have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Zeng S, Xue Y, Zhao J, Liu A, Zhang Z, Sun Y, et al. Total parenteral nutrition versus early enteral nutrition after cystectomy: a meta-analysis of postoperative outcomes. Int Urol Nephrol. 2019;51(1):1–7. - PubMed
-
- Heyland DK, Cook DJ, Guyatt GH. Enteral nutrition in the critically ill patient: a critical review of the evidence. Intensive Care Med. 1993;19(8):435–442. - PubMed
-
- Abdelgadir MA, Mahadi SE, Nasr AO, Ahmed ME. Role of jejunostomy feeding catheter as a model for nutritional support. Int J Surg. 2010;8(6):439–443. - PubMed
-
- Jenkinson AD, Lim J, Agrawal N, Menzies D. Laparoscopic feeding jejunostomy in esophagogastric cancer. Surg Endosc. 2007;21(2):299–302. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
