

Body mass index and waist circumference in relation to the risk of 26 types of cancer: a prospective cohort study of 3.5 million adults in Spain
- PMID: 33441148
- PMCID: PMC7807518
- DOI: 10.1186/s12916-020-01877-3
Body mass index and waist circumference in relation to the risk of 26 types of cancer: a prospective cohort study of 3.5 million adults in Spain
Abstract
Background: A high body mass index (BMI) has been associated with increased risk of several cancers; however, whether BMI is related to a larger number of cancers than currently recognized is unclear. Moreover, whether waist circumference (WC) is more strongly associated with specific cancers than BMI is not well established. We aimed to investigate the associations between BMI and 26 cancers accounting for non-linearity and residual confounding by smoking status as well as to compare cancer risk estimates between BMI and WC.
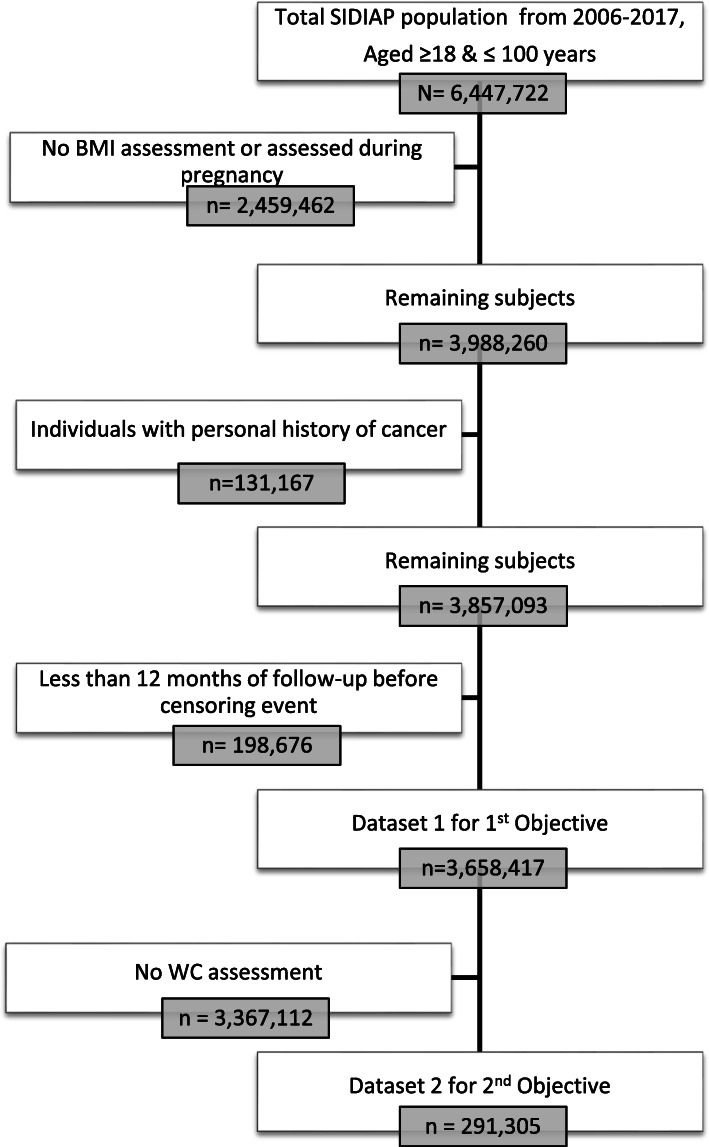
Methods: Prospective cohort study with population-based electronic health records from Catalonia, Spain. We included 3,658,417 adults aged ≥ 18 years and free of cancer at baseline between 2006 and 2017. Our main outcome measures were cause-specific hazard ratios (HRs) with 99% confidence intervals (CIs) for incident cancer at 26 anatomical sites.
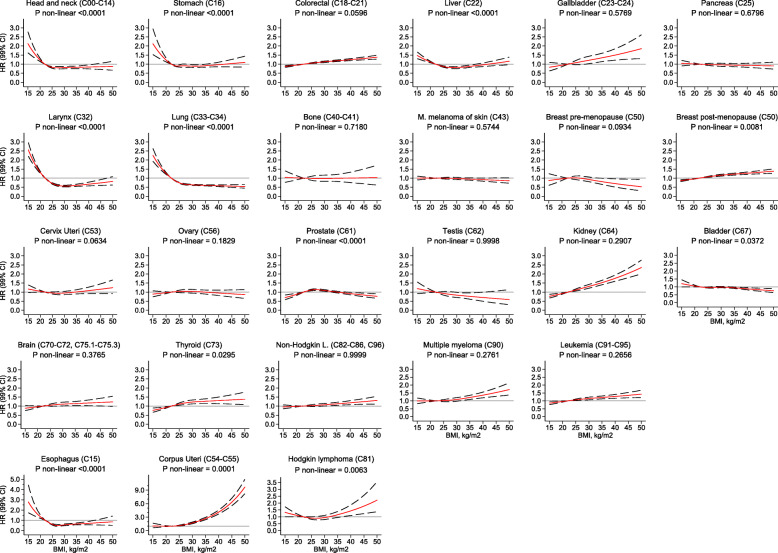
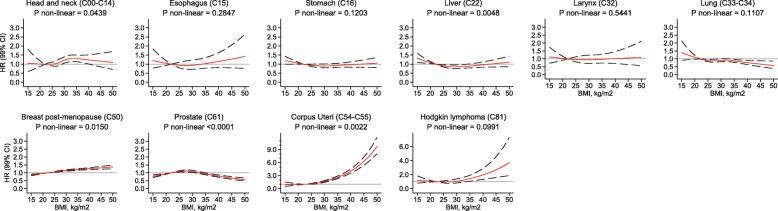
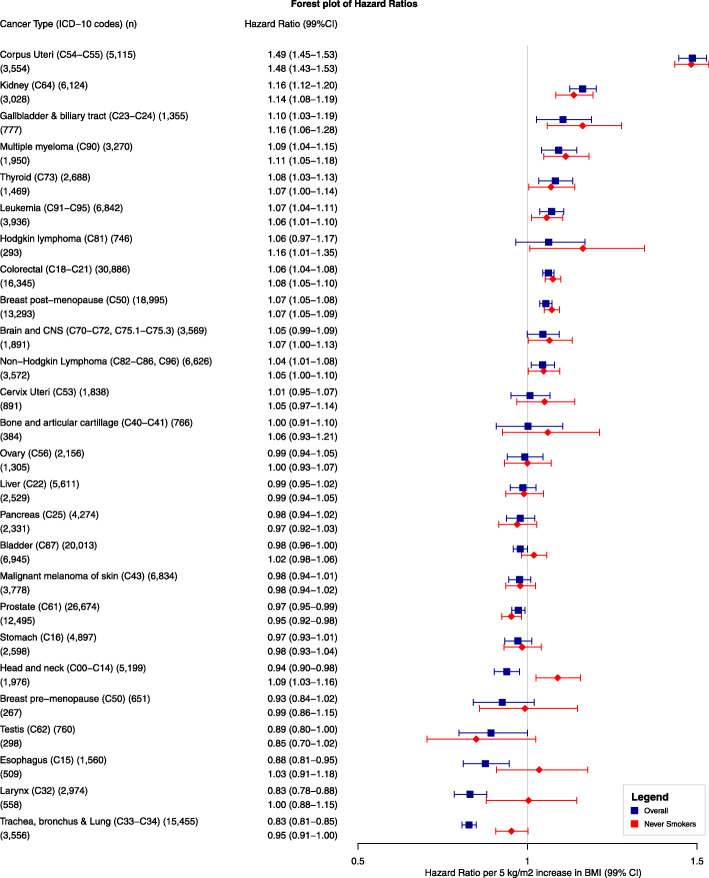
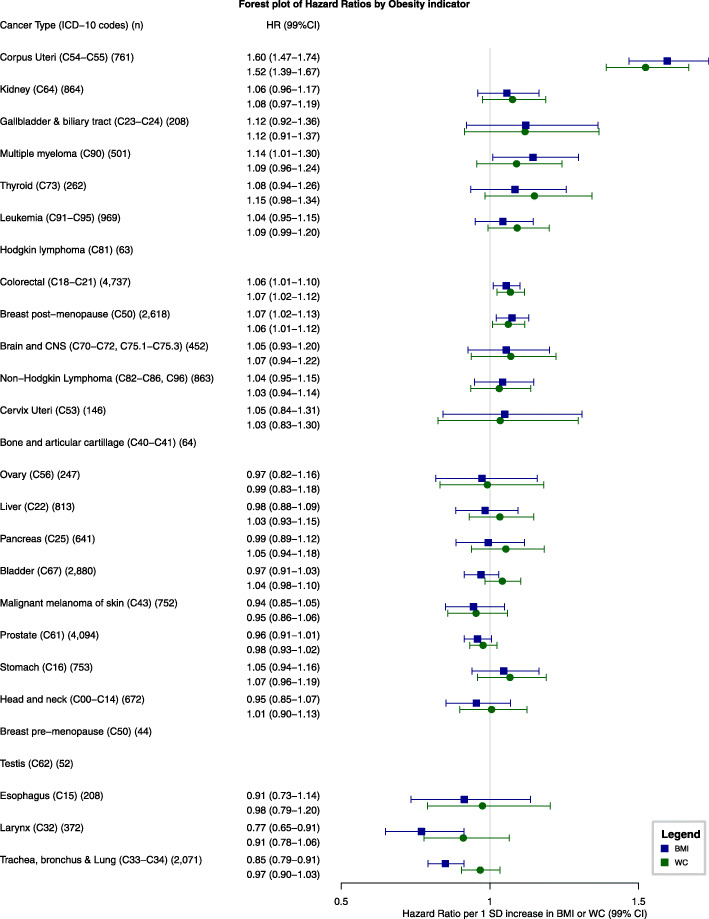
Results: After a median follow-up time of 8.3 years, 202,837 participants were diagnosed with cancer. A higher BMI was positively associated with risk of nine cancers (corpus uteri, kidney, gallbladder, thyroid, colorectal, breast post-menopausal, multiple myeloma, leukemia, non-Hodgkin lymphoma) and was positively associated with three additional cancers among never smokers (head and neck, brain and central nervous system, Hodgkin lymphoma). The respective HRs (per 5 kg/m2 increment) ranged from 1.04 (99%CI 1.01 to 1.08) for non-Hodgkin lymphoma to 1.49 (1.45 to 1.53) for corpus uteri cancer. While BMI was negatively associated to five cancer types in the linear analyses of the overall population, accounting for non-linearity revealed that BMI was associated to prostate cancer in a U-shaped manner and to head and neck, esophagus, larynx, and trachea, bronchus and lung cancers in an L-shaped fashion, suggesting that low BMIs are an approximation of heavy smoking. Of the 291,305 participants with a WC measurement, 27,837 were diagnosed with cancer. The 99%CIs of the BMI and WC point estimates (per 1 standard deviation increment) overlapped for all cancers.
Conclusions: In this large Southern European study, a higher BMI was associated with increased risk of twelve cancers, including four hematological and head and neck (only among never smokers) cancers. Furthermore, BMI and WC showed comparable estimates of cancer risk associated with adiposity.
Keywords: Adiposity; Body fat distribution; Body mass index; Body size; Cancer; Electronic health records; Obesity; Waist circumference.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- World Health Organization. Overweight and obesity. 2016 [cited 2018 Nov 5]. Available from: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
-
- Reeves GK, Pirie K, Beral V, Green J, Spencer E, Bull D. Cancer incidence and mortality in relation to body mass index in the Million Women Study: cohort study. Br Med J. 2007;335(7630):1134–1139. doi: 10.1136/bmj.39367.495995.AE. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
