

Symptom heterogeneity and patient subgroup classification among US patients with post-treatment Lyme disease: an observational study
- PMID: 33441353
- PMCID: PMC7812114
- DOI: 10.1136/bmjopen-2020-040399
Symptom heterogeneity and patient subgroup classification among US patients with post-treatment Lyme disease: an observational study
Abstract
Objectives: To identify underlying subgroups with distinct symptom profiles, and to characterise and compare these subgroups across a range of demographic, clinical and psychosocial factors, within a heterogeneous group of patients with well-defined post-treatment Lyme disease (PTLD).
Design: A clinical case series of patents.
Setting: Participants were recruited from a single-site, Lyme disease referral clinic patient population and were evaluated by physical exam, clinical laboratory testing and standardised questionnaires.
Participants: Two hundred and twelve participants met study criteria for PTLD, with medical record-confirmed prior Lyme disease as well as current symptoms and functional impact.
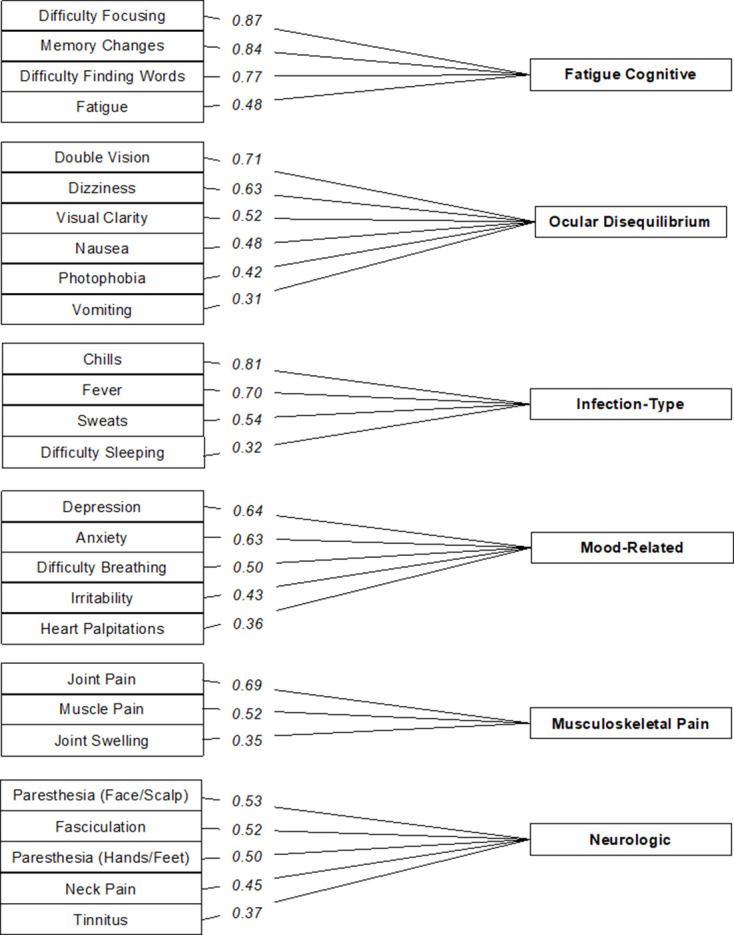
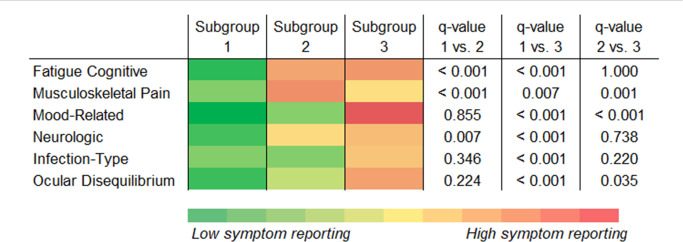
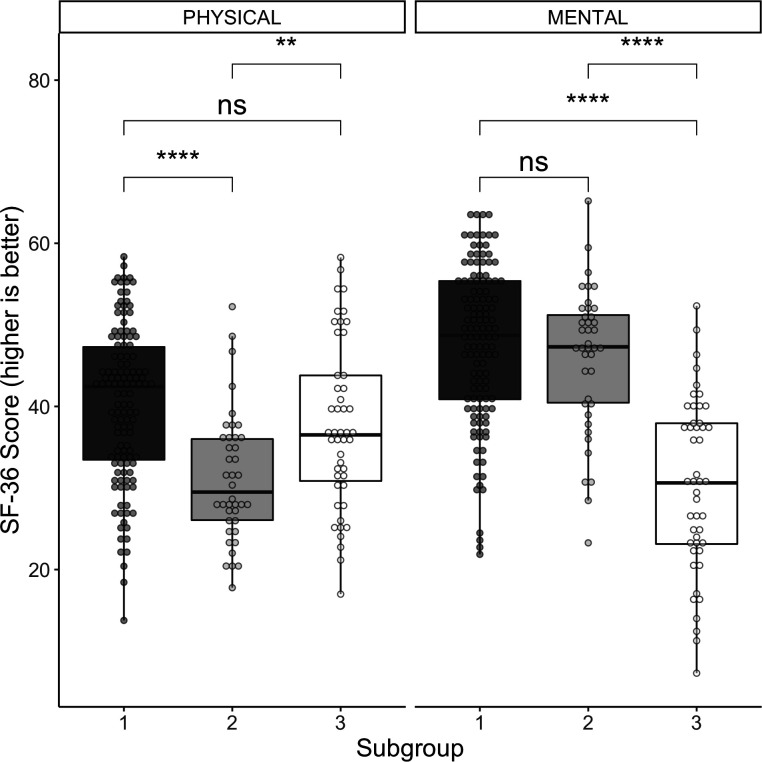
Results: Exploratory factor analysis classified 30 self-reported symptoms into 6 factors: 'Fatigue Cognitive', 'Ocular Disequilibrium', 'Infection-Type', 'Mood-Related', 'Musculoskeletal Pain' and 'Neurologic'. A final latent profile analysis was conducted using 'Fatigue Cognitive', 'Musculoskeletal Pain' and 'Mood-Related' factor-based scores, which produced three emergent symptom profiles, and participants were classified into corresponding subgroups with 59.0%, 18.9% and 22.2% of the sample, respectively. Compared with the other two groups, subgroup 1 had similarly low levels across all factors relative to the sample as a whole, and reported lower rates of disability (1.6% vs 10.0%, 12.8%; q=0.126, 0.035) and higher self-efficacy (median: 7.5 vs 6.0, 5.3; q=0.068,<0.001). Subgroup 2 had the highest 'Musculoskeletal Pain' factor-based scores (q≤0.001). Subgroup 3 was characterised overall by higher symptom factor-based scores, and reported higher depression (q≤0.001).
Conclusions: This analysis identified six symptom factors and three potentially clinically relevant subgroups among patients with well-characterised PTLD. We found that these subgroups were differentiated not only by symptom phenotype, but also by a range of other factors. This may serve as an initial step towards engaging with the symptom heterogeneity that has long been observed among patients with this condition.
Keywords: infectious diseases; internal medicine; primary care.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the infectious diseases Society of America. Clin Infect Dis 2006;43:1089–134. 10.1086/508667 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous