

Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials
- PMID: 33441402
- PMCID: PMC7804890
- DOI: 10.1136/bmj.m4573
Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials
Erratum in
-
Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials.BMJ. 2022 Jan 18;376:o109. doi: 10.1136/bmj.o109. BMJ. 2022. PMID: 35044930 Free PMC article. No abstract available.
Abstract
Objective: To evaluate sodium-glucose cotransporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists in patients with type 2 diabetes at varying cardiovascular and renal risk.
Design: Network meta-analysis.
Data sources: Medline, Embase, and Cochrane CENTRAL up to 11 August 2020.
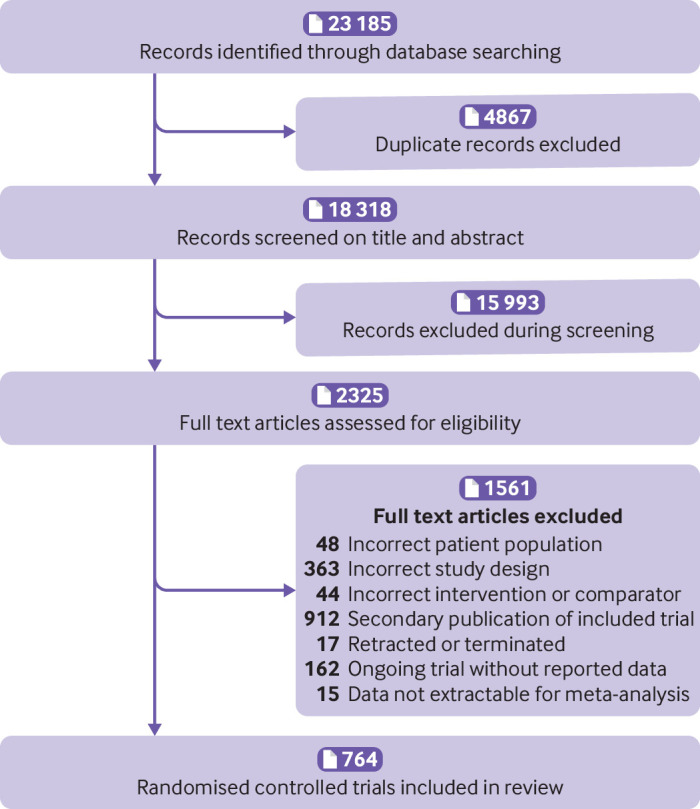
Eligibility criteria for selecting studies: Randomised controlled trials comparing SGLT-2 inhibitors or GLP-1 receptor agonists with placebo, standard care, or other glucose lowering treatment in adults with type 2 diabetes with follow up of 24 weeks or longer. Studies were screened independently by two reviewers for eligibility, extracted data, and assessed risk of bias.
Main outcome measures: Frequentist random effects network meta-analysis was carried out and GRADE (grading of recommendations assessment, development, and evaluation) used to assess evidence certainty. Results included estimated absolute effects of treatment per 1000 patients treated for five years for patients at very low risk (no cardiovascular risk factors), low risk (three or more cardiovascular risk factors), moderate risk (cardiovascular disease), high risk (chronic kidney disease), and very high risk (cardiovascular disease and kidney disease). A guideline panel provided oversight of the systematic review.
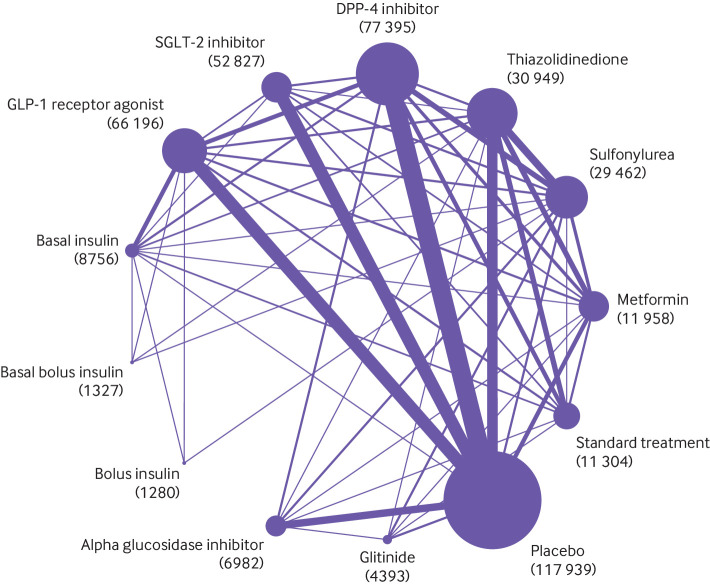
Results: 764 trials including 421 346 patients proved eligible. All results refer to the addition of SGLT-2 inhibitors and GLP-1 receptor agonists to existing diabetes treatment. Both classes of drugs lowered all cause mortality, cardiovascular mortality, non-fatal myocardial infarction, and kidney failure (high certainty evidence). Notable differences were found between the two agents: SGLT-2 inhibitors reduced admission to hospital for heart failure more than GLP-1 receptor agonists, and GLP-1 receptor agonists reduced non-fatal stroke more than SGLT-2 inhibitors (which appeared to have no effect). SGLT-2 inhibitors caused genital infection (high certainty), whereas GLP-1 receptor agonists might cause severe gastrointestinal events (low certainty). Low certainty evidence suggested that SGLT-2 inhibitors and GLP-1 receptor agonists might lower body weight. Little or no evidence was found for the effect of SGLT-2 inhibitors or GLP-1 receptor agonists on limb amputation, blindness, eye disease, neuropathic pain, or health related quality of life. The absolute benefits of these drugs vary substantially across patients from low to very high risk of cardiovascular and renal outcomes (eg, SGLT-2 inhibitors resulted in 3 to 40 fewer deaths in 1000 patients over five years; see interactive decision support tool (https://magicevidence.org/match-it/200820dist/#!/) for all outcomes.
Conclusions: In patients with type 2 diabetes, SGLT-2 inhibitors and GLP-1 receptor agonists reduced cardiovascular and renal outcomes, with some differences in benefits and harms. Absolute benefits are determined by individual risk profiles of patients, with clear implications for clinical practice, as reflected in the BMJ Rapid Recommendations directly informed by this systematic review.
Systematic review registration: PROSPERO CRD42019153180.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: SCP, BT, RAM, POV, SL, QH, DT, MR, PN, VS, YC, ACNF, MB, LIF, AL, NA, YL, ST, TM, NK, RDB, RM, AKRC, HW, XC, XZ, JL, AFR, ADGC, YW, LL, SS, RCS, FDG, RRG, MW, GG, GFMS: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. SL was supported by grants from the National Natural Science Foundation of China (grant number 21534008), Sichuan Science and Technology Programme (grant number 2019YFH0150), and 1.3.5 Project for Disciplines of Excellence, West China Hospital, Sichuan University (grant numbers ZYGD18022 and 2020HXF011). None of these grants contribute to this work. AN reports grants and personal fees from Novo Nordisk, grants from Sanofi, grants and personal fees from Astra Zeneca, grants from Pikdare, grants from AlfaSigma, outside the submitted work. DWJ reports grants and personal fees from Baxter Healthcare, grants and personal fees from Fresenius Medical Care, other from Amgen, personal fees from Astra Zeneca, personal fees from AWAK, grants from National Health and Medical Research Council of Australia, personal fees from Ono, outside the submitted work. MT reports a grant to the institution by Daichi Sankyo in lieu of a personal honorarium. MCR reports grants from Sanofi, grants from NovoNordisk, grants from AstraZeneca, grants from Pikdare, during the conduct of the study. SVB reports advisory board membership to Bayer Australia and AstraZeneca, speaking honoraria from Bayer Australia and Pfizer Australia; non-financial research support from Bayer AG. LG reports personal fees from Boehringer-Engelheim, personal fees from Lilly, personal fees from Astra Zeneca, non-financial support from Novo Nordisk, outside the submitted work.
Figures
Comment in
-
In type 2 diabetes, SGLT2 inhibitors reduce all-cause, but not cardiovascular, mortality vs. GLP-1 RAs.Ann Intern Med. 2021 Jun;174(6):JC67. doi: 10.7326/ACPJ202106150-067. Epub 2021 Jun 1. Ann Intern Med. 2021. PMID: 34058114
References
-
- World Health Organization. Global Health Observatory (GHO) data. https://www.who.int/data/gho/data/themes/topics/causes-of-death. World Health Organization, Geneva, Switzerland.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical