

Specific Norovirus Interaction with Lewis x and Lewis a on Human Intestinal Inflammatory Mucosa during Refractory Inflammatory Bowel Disease
- PMID: 33441404
- PMCID: PMC7845605
- DOI: 10.1128/mSphere.01185-20
Specific Norovirus Interaction with Lewis x and Lewis a on Human Intestinal Inflammatory Mucosa during Refractory Inflammatory Bowel Disease
Abstract
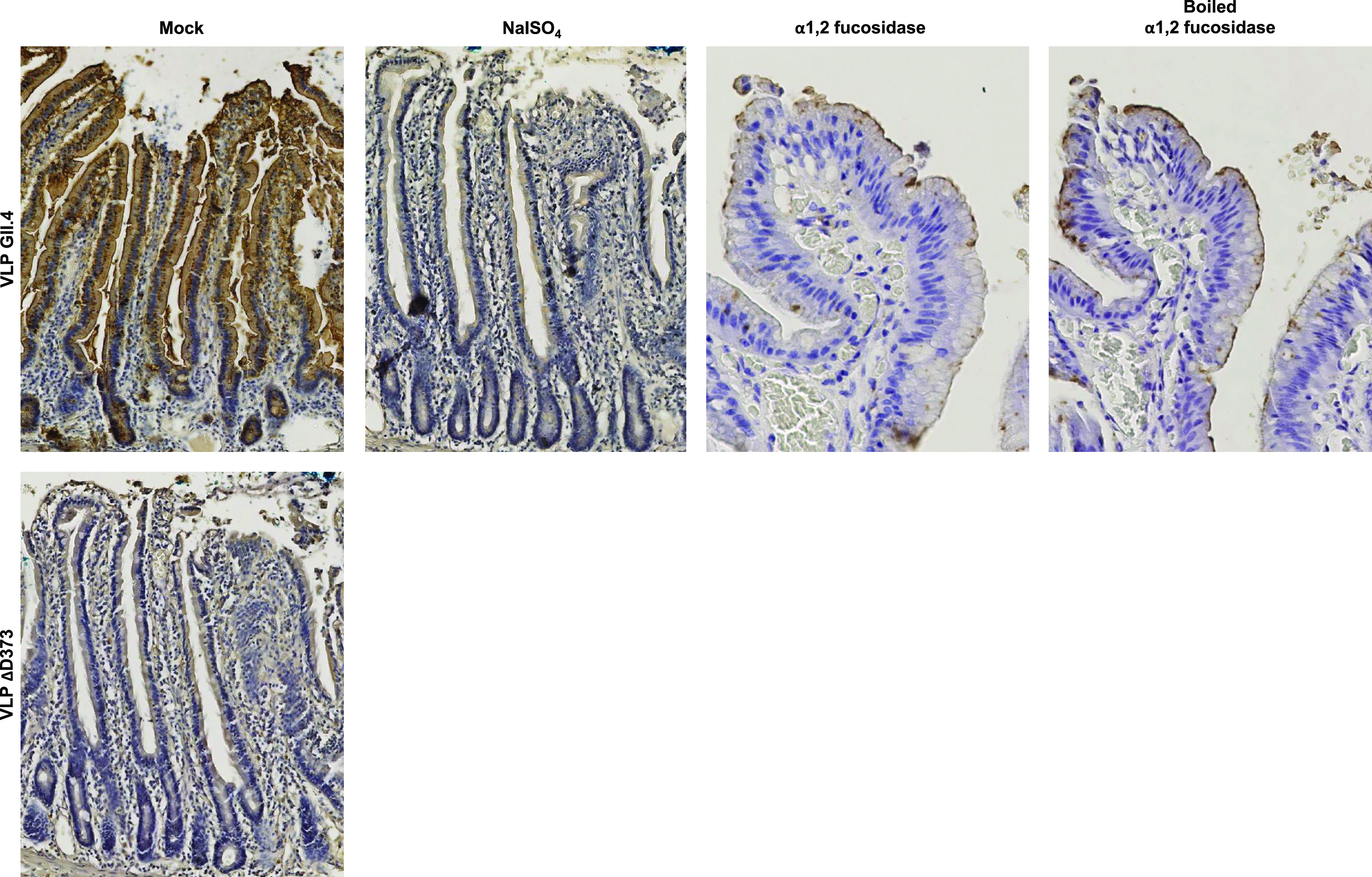
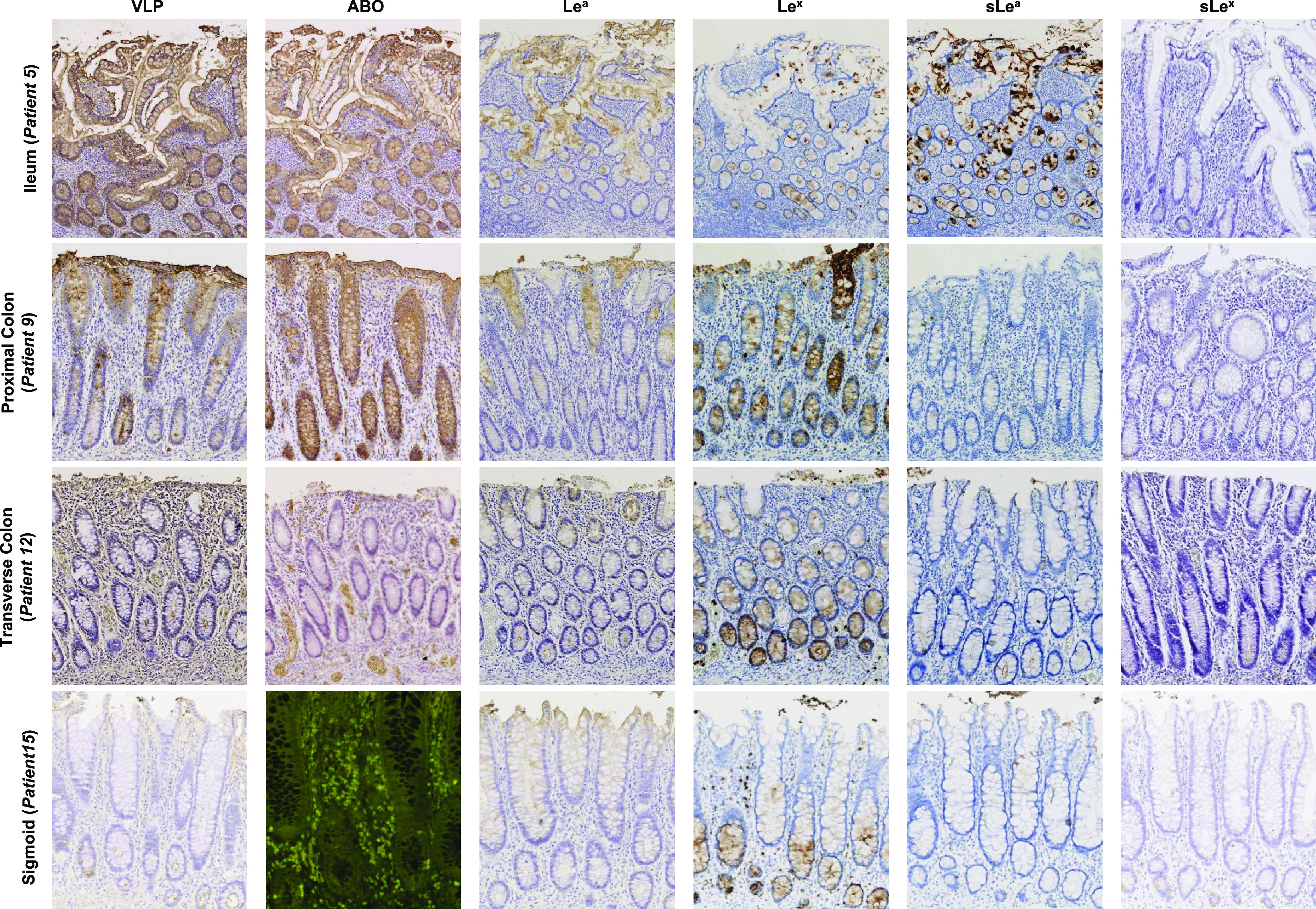
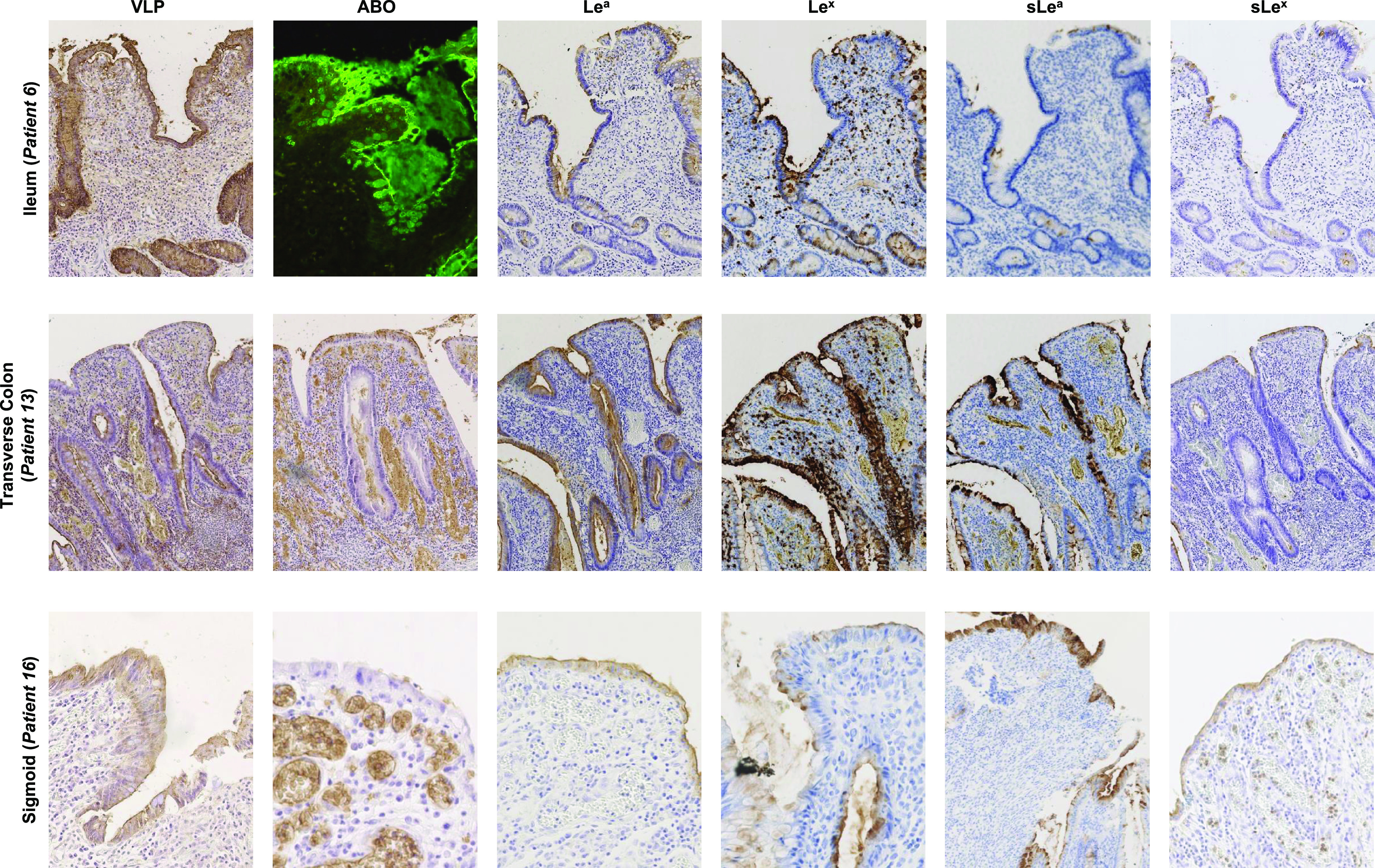
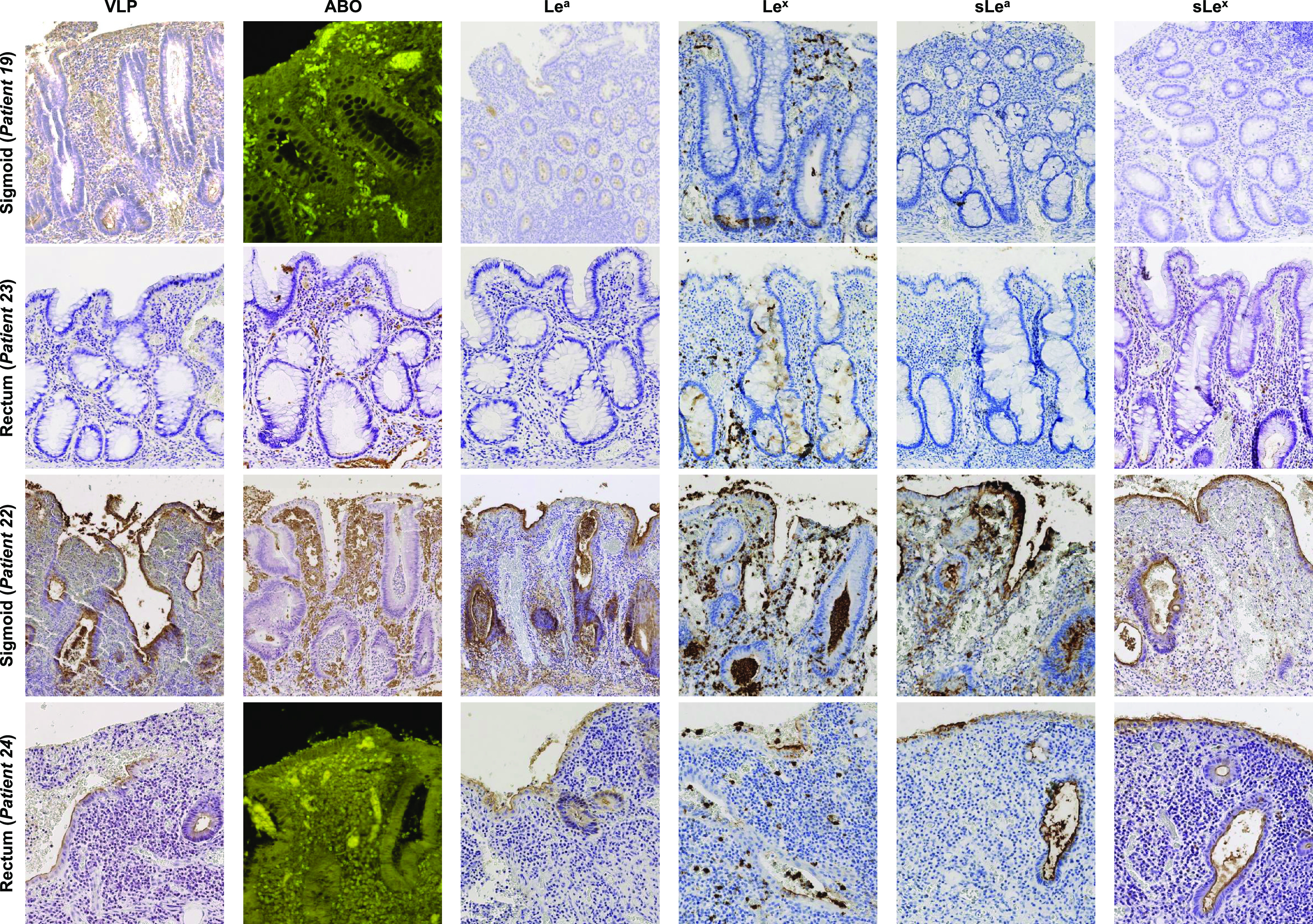
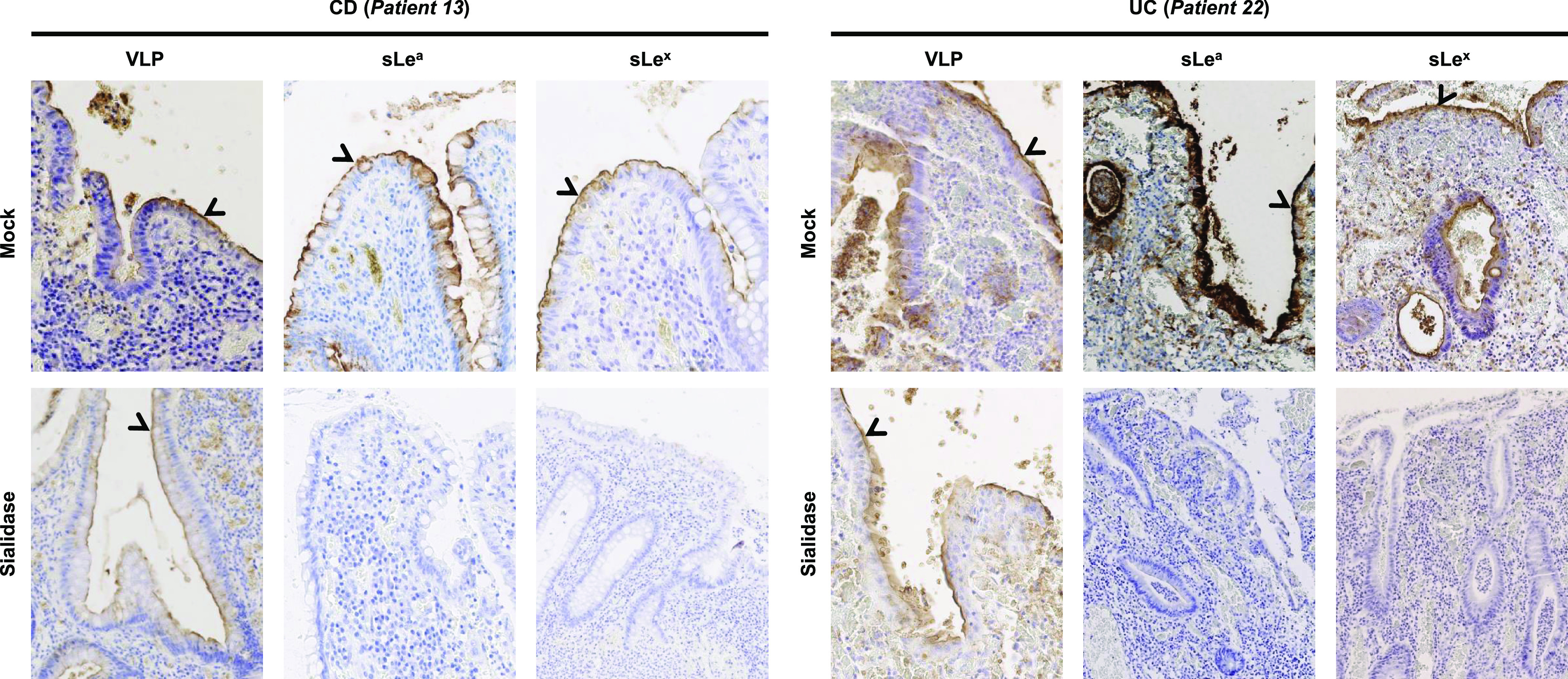
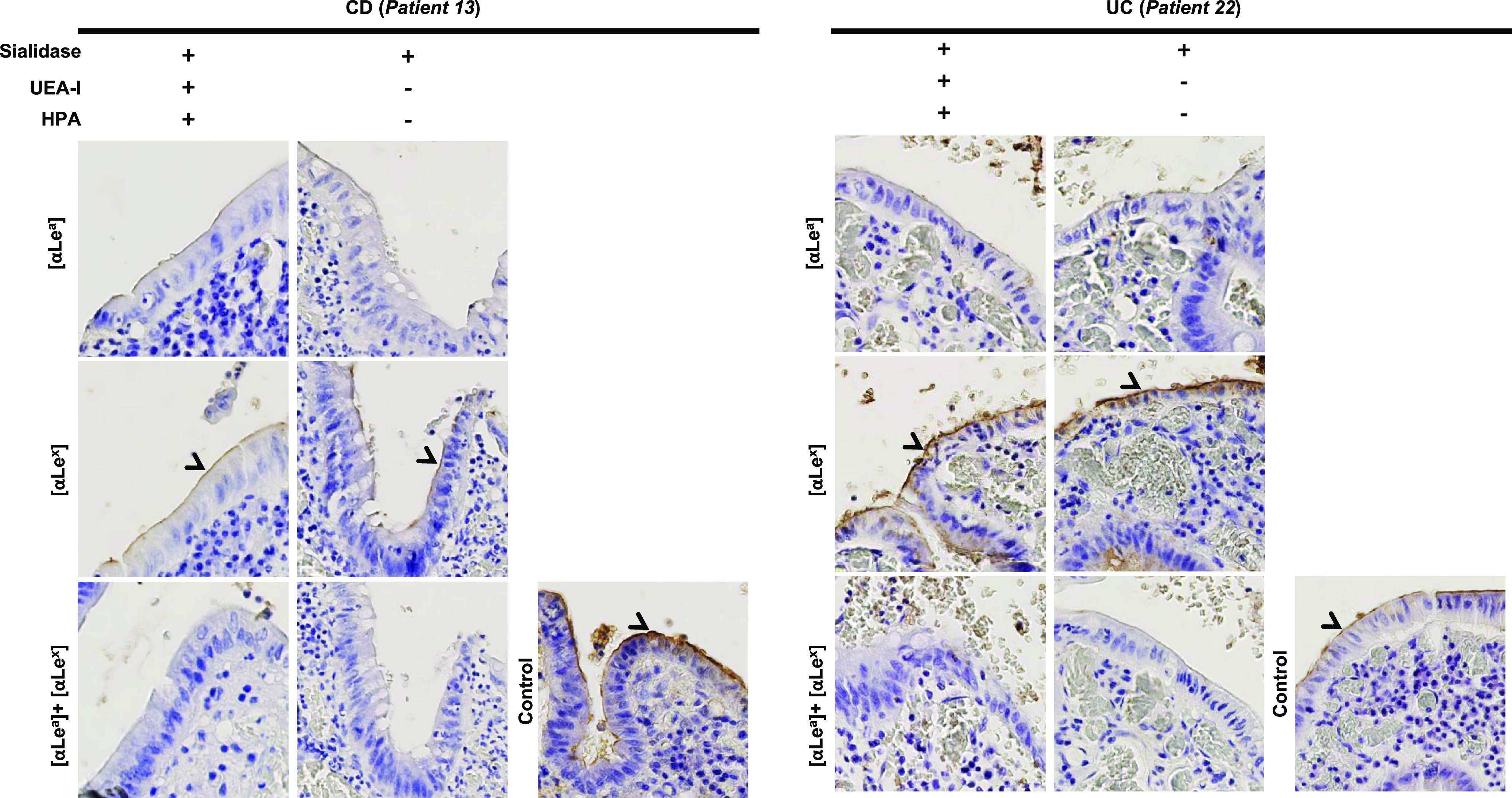
Inflammatory bowel disease (IBD), which includes Crohn's disease (CD) and ulcerative colitis (UC), is related to immunological and microbial factors, with the possible implication of enteric viruses. We characterized the interaction between human noroviruses (HuNoVs) and blood group antigens in refractory CD and UC using HuNoV virus-like particles (VLPs) and histological tissues. Immunohistochemistry was conducted on inflammatory tissue samples from the small intestine, colon, and rectum in 15 CD and 9 UC patients. Analysis of the regenerative mucosa of the colon and rectum revealed strong expression of sialylated Lewis a (sLea) and Lewis x (sLex) antigens and HuNoV VLP binding in the absence of ABO antigen expression in both UC and CD. Competition experiments using sialidase, lectins, and monoclonal antibodies demonstrated that HuNoV attachment mostly involved Lea and, to a lesser extent, Lex moieties on regenerative mucosa in both UC and CD. Further studies will be required to understand the implications of specific HuNoV binding to regenerative mucosa in refractory IBD.IMPORTANCE Inflammatory bowel diseases (IBD), including Crohn's disease (CD) and ulcerative colitis (UC), are progressive diseases affecting millions of people each year. Flare-ups during IBD result in severe mucosal alterations of the small intestine (in CD) and in the colon and rectum (in CD and UC). Immunohistochemical analysis of CD and UC samples showed strong expression of known tumoral markers sialyl Lewis a (CA19.9) and sialyl Lewis x (CD15s) antigens on colonic and rectal regenerative mucosa, concurrent with strong human norovirus (HuNov) VLP GII.4 affinity. Sialidase treatment and competition experiments using histo-blood group antigen (HBGA)-specific monoclonal antibodies and lectins clearly demonstrated the implication of the Lewis a moiety and, to a lesser extent, the Lewis x moiety in HuNov recognition in regenerative mucosa of CD and UC tissues. Further studies are required to explore the possible implications of enteric viruses in the impairment of epithelial repair and dysregulation of inflammatory pathways during severe IBD.
Keywords: Crohn’s disease; HBGA; gut inflammation; inflammation; norovirus; ulcerative colitis.
Copyright © 2021 Tarris et al.
Figures
Similar articles
-
Intestinal Norovirus Binding Patterns in Nonsecretor Individuals.J Virol. 2022 Oct 12;96(19):e0086522. doi: 10.1128/jvi.00865-22. Epub 2022 Sep 19. J Virol. 2022. PMID: 36121297 Free PMC article.
-
Development, validation and implementation of an in vitro model for the study of metabolic and immune function in normal and inflamed human colonic epithelium.Dan Med J. 2015 Jan;62(1):B4973. Dan Med J. 2015. PMID: 25557335 Review.
-
CD40 and CD86 upregulation with divergent CMRF44 expression on blood dendritic cells in inflammatory bowel diseases.Am J Gastroenterol. 2001 Oct;96(10):2946-56. doi: 10.1111/j.1572-0241.2001.04686.x. Am J Gastroenterol. 2001. PMID: 11693331
-
Human intestinal organoids express histo-blood group antigens, bind norovirus VLPs, and support limited norovirus replication.Sci Rep. 2017 Oct 3;7(1):12621. doi: 10.1038/s41598-017-12736-2. Sci Rep. 2017. PMID: 28974702 Free PMC article.
-
Enteric Viruses and Inflammatory Bowel Disease.Viruses. 2021 Jan 13;13(1):104. doi: 10.3390/v13010104. Viruses. 2021. PMID: 33451106 Free PMC article. Review.
Cited by
-
Epidemiological Impact of GII.17 Human Noroviruses Associated With Attachment to Enterocytes.Front Microbiol. 2022 Apr 27;13:858245. doi: 10.3389/fmicb.2022.858245. eCollection 2022. Front Microbiol. 2022. PMID: 35572680 Free PMC article.
-
Association Between Inflammatory Bowel Disease and Viral Infections.Curr Microbiol. 2023 Apr 27;80(6):195. doi: 10.1007/s00284-023-03305-0. Curr Microbiol. 2023. PMID: 37106245 Free PMC article. Review.
-
Determining the Importance of Carbohydrate-Based Structures in Murine Norovirus Binding to Commensal Bacteria.Viruses. 2025 Aug 20;17(8):1142. doi: 10.3390/v17081142. Viruses. 2025. PMID: 40872855 Free PMC article.
-
Finding the sweet spot: glycosylation mediated regulation of intestinal inflammation.Mucosal Immunol. 2022 Feb;15(2):211-222. doi: 10.1038/s41385-021-00466-8. Epub 2021 Nov 15. Mucosal Immunol. 2022. PMID: 34782709 Free PMC article. Review.
-
Intestinal Norovirus Binding Patterns in Nonsecretor Individuals.J Virol. 2022 Oct 12;96(19):e0086522. doi: 10.1128/jvi.00865-22. Epub 2022 Sep 19. J Virol. 2022. PMID: 36121297 Free PMC article.
References
-
- Fenoglio-Preiser CM, Noffsinger AE, Stemmermann GN, Lantz PE, Isaacson PG. 2008. Gastrointestinal pathology, 3rd ed, p 593–690. Lippincott Williams & Wilkins, Philadelphia, PA.
-
- Theodoratou E, Campbell H, Ventham NT, Kolarich D, Pucic-Bakovic M, Zoldos V, Fernandes D, Pemberton IK, Rudan I, Kennedy NA, Wuhrer M, Nimmo E, Annese V, McGovern DP, Satsangi J, Lauc G. 2014. The role of glycosylation in IBD. Nat Rev Gastroenterol Hepatol 11:588–600. doi:10.1038/nrgastro.2014.78. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
