

Randomized Controlled Trial of Oral Vancomycin Treatment in Clostridioides difficile-Colonized Patients
- PMID: 33441409
- PMCID: PMC7845614
- DOI: 10.1128/mSphere.00936-20
Randomized Controlled Trial of Oral Vancomycin Treatment in Clostridioides difficile-Colonized Patients
Abstract
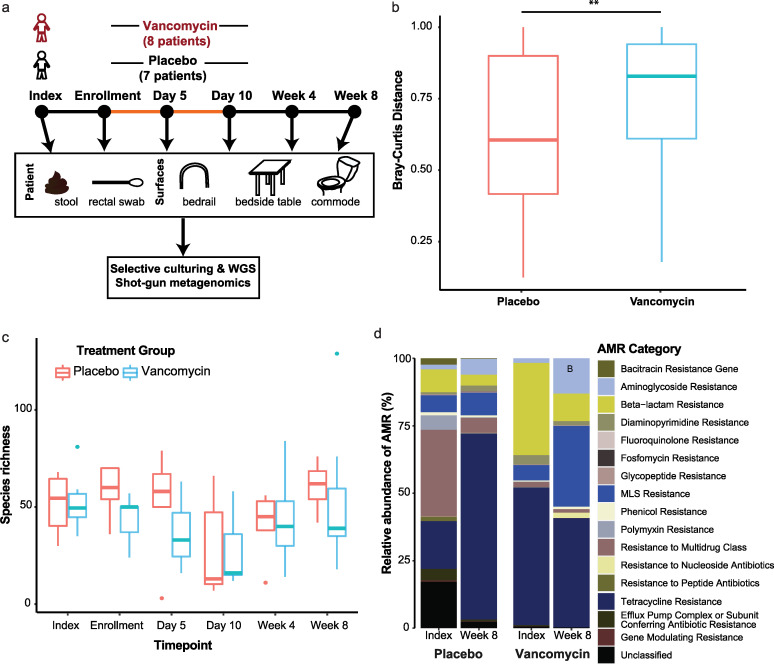
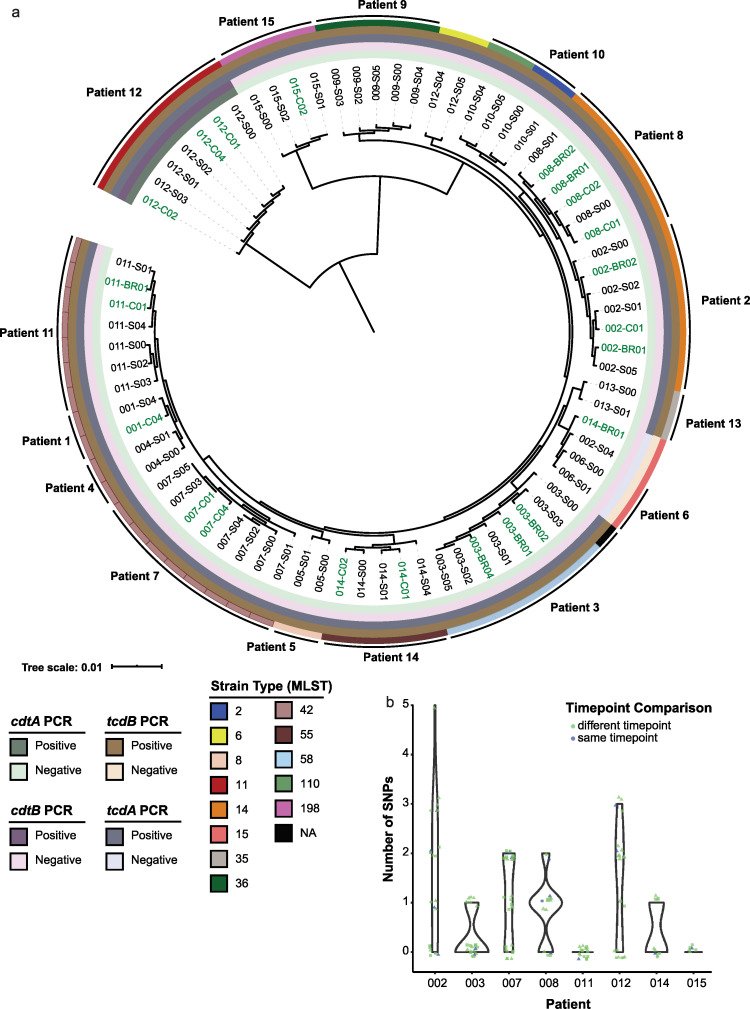
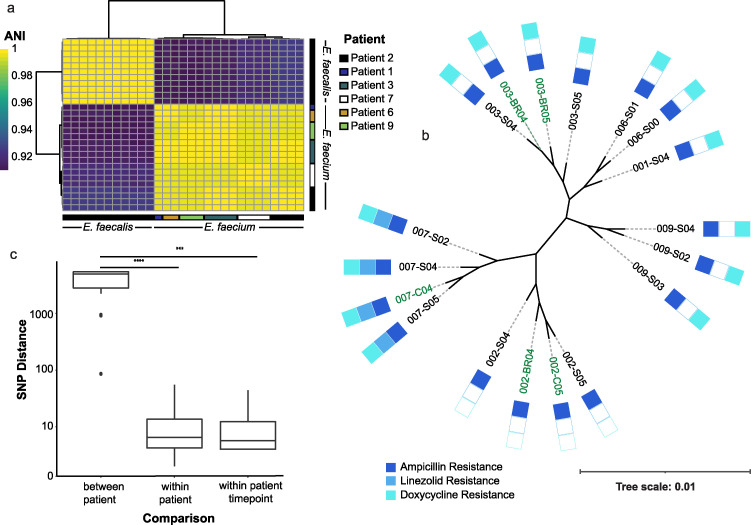
Clostridioides difficile infection (CDI) is most commonly diagnosed using nucleic acid amplification tests (NAAT); the low positive predictive value of these assays results in patients colonized with C. difficile unnecessarily receiving CDI treatment antibiotics. The risks and benefits of antibiotic treatment in individuals with such cases are unknown. Fecal samples of NAAT-positive, toxin enzyme immunoassay (EIA)-negative patients were collected before, during, and after randomization to vancomycin (n = 8) or placebo (n = 7). C. difficile and antibiotic-resistant organisms (AROs) were selectively cultured from fecal and environmental samples. Shotgun metagenomics and comparative isolate genomics were used to understand the impact of oral vancomycin on the microbiome and environmental contamination. Overall, 80% of placebo patients and 71% of vancomycin patients were colonized with C. difficile posttreatment. One person randomized to placebo subsequently received treatment for CDI. In the vancomycin-treated group, beta-diversity (P = 0.0059) and macrolide-lincosamide-streptogramin (MLS) resistance genes (P = 0.037) increased after treatment; C. difficile and vancomycin-resistant enterococci (VRE) environmental contamination was found in 53% of patients and 26% of patients, respectively. We found that vancomycin alters the gut microbiota, does not permanently clear C. difficile, and is associated with VRE colonization/environmental contamination. (This study has been registered at ClinicalTrials.gov under registration no. NCT03388268.)IMPORTANCE A gold standard diagnostic for Clostridioides difficile infection (CDI) does not exist. An area of controversy is how to manage patients whose stool tests positive by nucleic acid amplification tests but negative by toxin enzyme immunoassay. Existing data suggest most of these patients do not have CDI, but most are treated with oral vancomycin. Potential benefits to treatment include a decreased risk for adverse outcomes if the patient does have CDI and the potential to decrease C. difficile shedding/transmission. However, oral vancomycin perturbs the intestinal microbiota and promotes antibiotic-resistant organism colonization/transmission. We conducted a double-blinded randomized controlled trial to assess the risk-benefit of oral vancomycin treatment in this population. Oral vancomycin did not result in long-term clearance of C. difficile, perturbed the microbiota, and was associated with colonization/shedding of vancomycin-resistant enterococci. This work underscores the need to better understand this population of patients in the context of C. difficile/ARO-related outcomes and transmission.
Keywords: C. difficile; vancomycin; vancomycin-resistant enterococci.
Copyright © 2021 Fishbein et al.
Figures
Comment in
-
Uncovering the Harms of Treating Clostridioides difficile Colonization.mSphere. 2021 Jan 13;6(1):e01296-20. doi: 10.1128/mSphere.01296-20. mSphere. 2021. PMID: 33441413 Free PMC article.
References
-
- Guh AY, Mu Y, Winston LG, Johnston H, Olson D, Farley MM, Wilson LE, Holzbauer SM, Phipps EC, Dumyati GK, Beldavs ZG, Kainer MA, Karlsson M, Gerding DN, McDonald LC, Emerging Infections Program Clostridioides difficile Infection Working Group. 2020. Trends in U.S. burden of Clostridioides difficile infection and outcomes. N Engl J Med 382:1320–1330. doi:10.1056/NEJMoa1910215. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
