

Immune modulation resulting from MR-guided high intensity focused ultrasound in a model of murine breast cancer
- PMID: 33441763
- PMCID: PMC7806949
- DOI: 10.1038/s41598-020-80135-1
Immune modulation resulting from MR-guided high intensity focused ultrasound in a model of murine breast cancer
Abstract
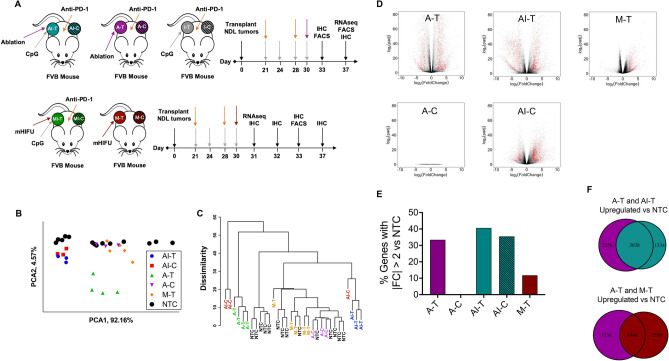
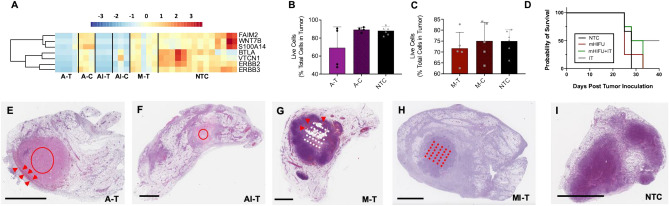
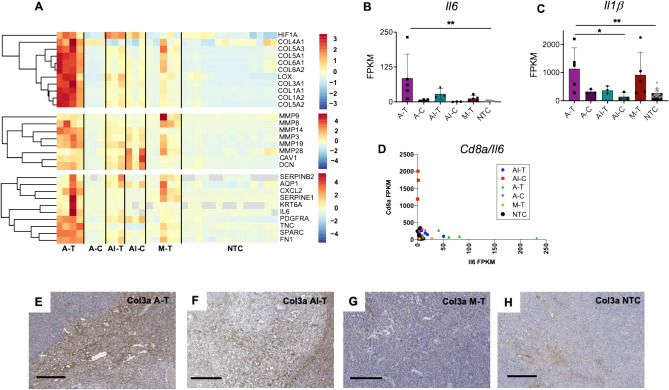
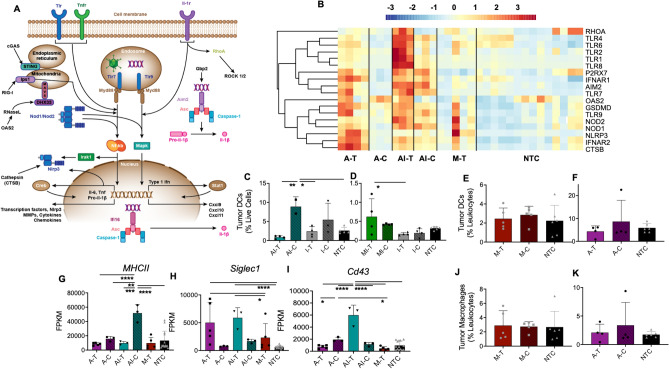
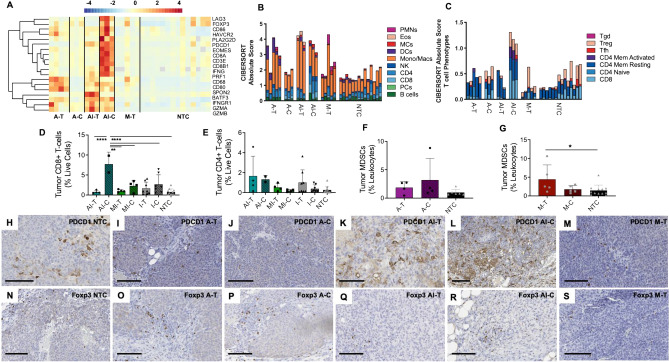
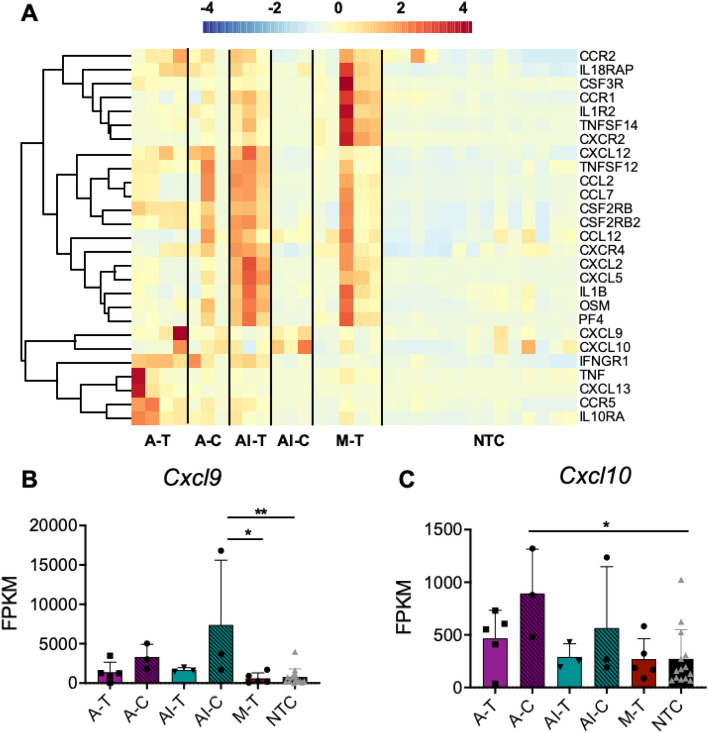
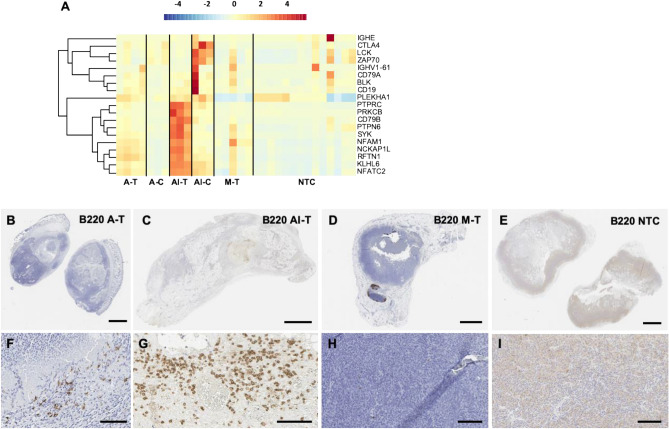
High intensity focused ultrasound (HIFU) rapidly and non-invasively destroys tumor tissue. Here, we sought to assess the immunomodulatory effects of MR-guided HIFU and its combination with the innate immune agonist CpG and checkpoint inhibitor anti-PD-1. Mice with multi-focal breast cancer underwent ablation with a parameter set designed to achieve mechanical disruption with minimal thermal dose or a protocol in which tumor temperature reached 65 °C. Mice received either HIFU alone or were primed with the toll-like receptor 9 agonist CpG and the checkpoint modulator anti-PD-1. Both mechanical HIFU and thermal ablation induced a potent inflammatory response with increased expression of Nlrp3, Jun, Mefv, Il6 and Il1β and alterations in macrophage polarization compared to control. Furthermore, HIFU upregulated multiple innate immune receptors and immune pathways, including Nod1, Nlrp3, Aim2, Ctsb, Tlr1/2/4/7/8/9, Oas2, and RhoA. The inflammatory response was largely sterile and consistent with wound-healing. Priming with CpG attenuated Il6 and Nlrp3 expression, further upregulated expression of Nod2, Oas2, RhoA, Pycard, Tlr1/2 and Il12, and enhanced T-cell number and activation while polarizing macrophages to an anti-tumor phenotype. The tumor-specific antigen, cytokines and cell debris liberated by HIFU enhance response to innate immune agonists.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
