

Functional connectome differences in individuals with hallucinations across the psychosis continuum
- PMID: 33441965
- PMCID: PMC7806763
- DOI: 10.1038/s41598-020-80657-8
Functional connectome differences in individuals with hallucinations across the psychosis continuum
Erratum in
-
Author Correction: Functional connectome differences in individuals with hallucinations across the psychosis continuum.Sci Rep. 2021 Apr 14;11(1):8540. doi: 10.1038/s41598-021-87849-w. Sci Rep. 2021. PMID: 33854185 Free PMC article. No abstract available.
Abstract
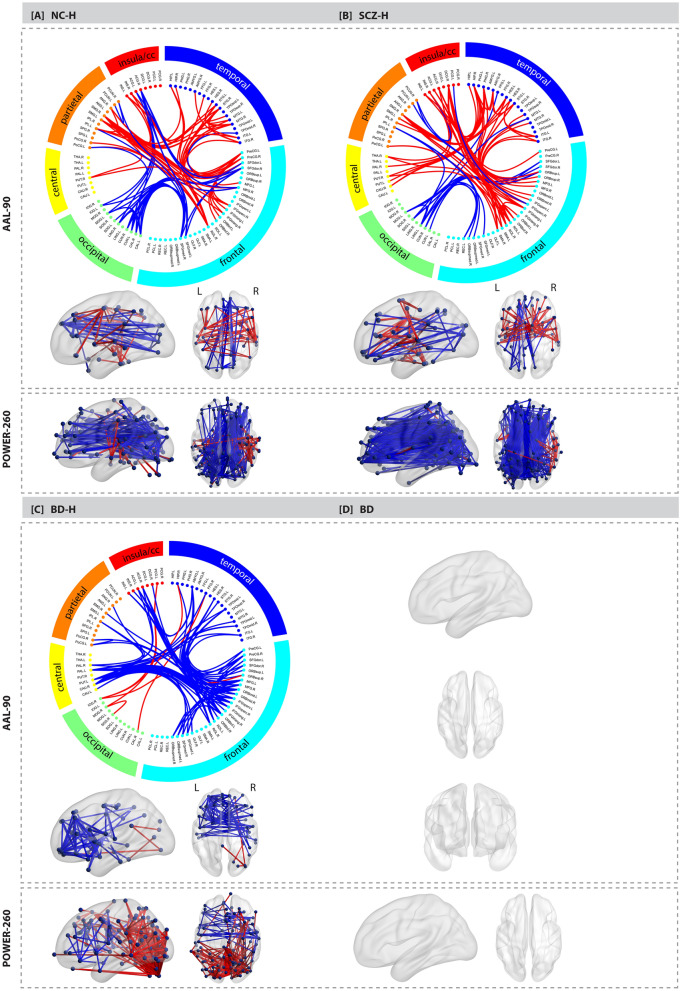
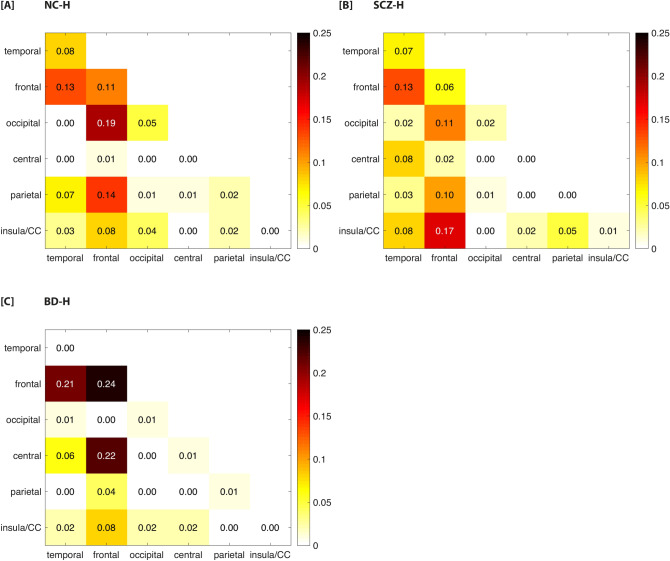
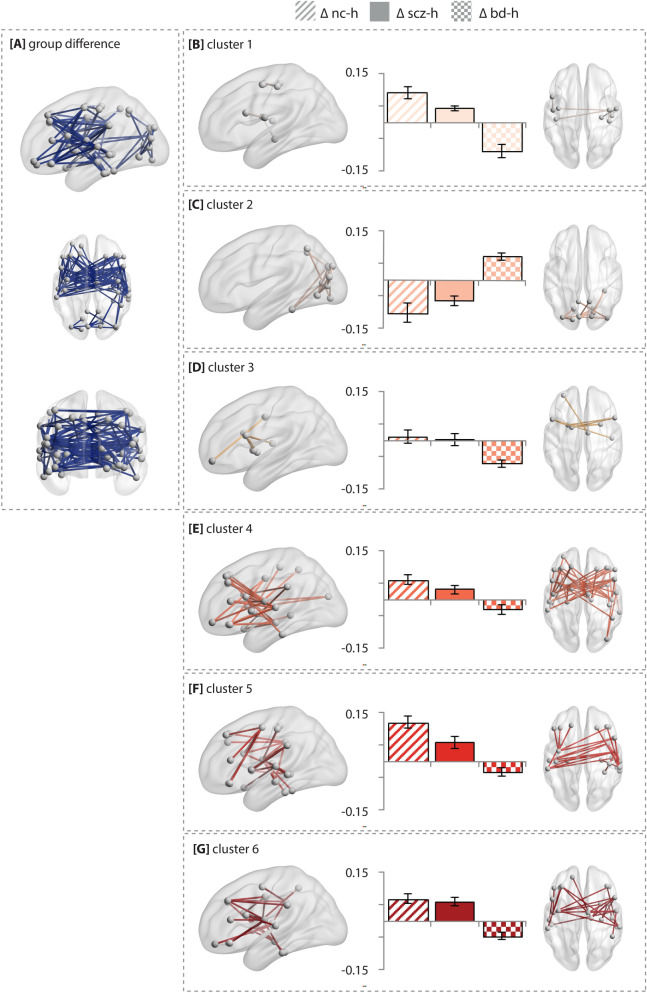
Hallucinations may arise from an imbalance between sensory and higher cognitive brain regions, reflected by alterations in functional connectivity. It is unknown whether hallucinations across the psychosis continuum exhibit similar alterations in functional connectivity, suggesting a common neural mechanism, or whether different mechanisms link to hallucinations across phenotypes. We acquired resting-state functional MRI scans of 483 participants, including 40 non-clinical individuals with hallucinations, 99 schizophrenia patients with hallucinations, 74 bipolar-I disorder patients with hallucinations, 42 bipolar-I disorder patients without hallucinations, and 228 healthy controls. The weighted connectivity matrices were compared using network-based statistics. Non-clinical individuals with hallucinations and schizophrenia patients with hallucinations exhibited increased connectivity, mainly among fronto-temporal and fronto-insula/cingulate areas compared to controls (P < 0.001 adjusted). Differential effects were observed for bipolar-I disorder patients with hallucinations versus controls, mainly characterized by decreased connectivity between fronto-temporal and fronto-striatal areas (P = 0.012 adjusted). No connectivity alterations were found between bipolar-I disorder patients without hallucinations and controls. Our results support the notion that hallucinations in non-clinical individuals and schizophrenia patients are related to altered interactions between sensory and higher-order cognitive brain regions. However, a different dysconnectivity pattern was observed for bipolar-I disorder patients with hallucinations, which implies a different neural mechanism across the psychosis continuum.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Sommer IE, Koops S, Blom JD. Comparison of auditory hallucinations across different disorders and syndromes. Neuropsychiatry. 2012;2:1–12. doi: 10.2217/npy.12.2. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
