

MICS CABG: a single-center experience of the first 100 cases
- PMID: 33442204
- PMCID: PMC7778645
- DOI: 10.1007/s12055-020-01048-2
MICS CABG: a single-center experience of the first 100 cases
Abstract
Purpose: To study the learning curve and outcomes of the first 100 cases of minimally invasive cardiac surgery (MICS) coronary artery bypass grafting (CABG) performed at our center.
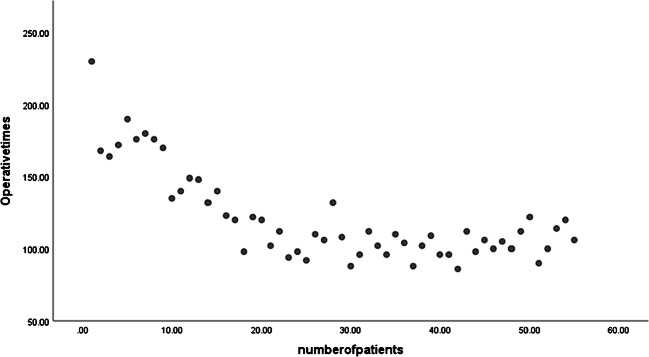
Methods: From January 2017 to November 2019, a total of 100 patients underwent CABG via left anterior thoracotomy approach. We have studied the operative times within the MICS CABG patients to analyze our learning curve. We also studied the postoperative outcomes and compared these with those of patients who underwent sternotomy during the same period.
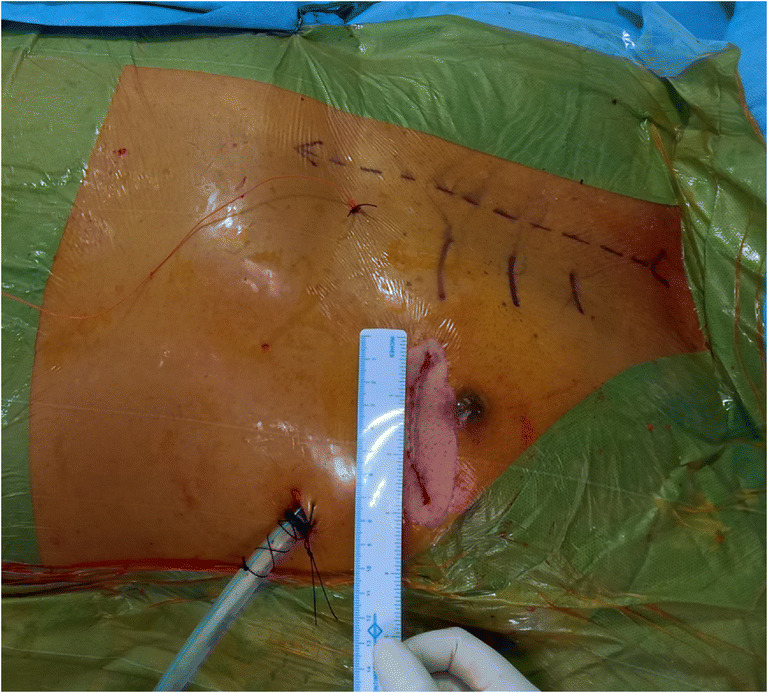
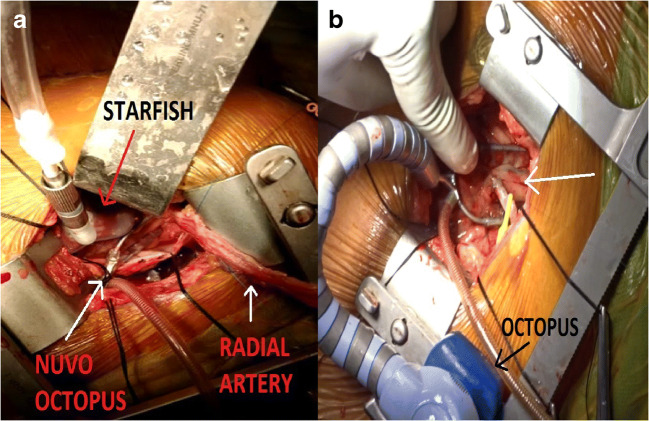
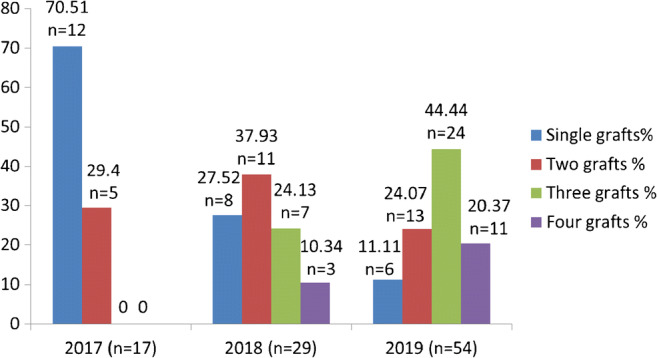
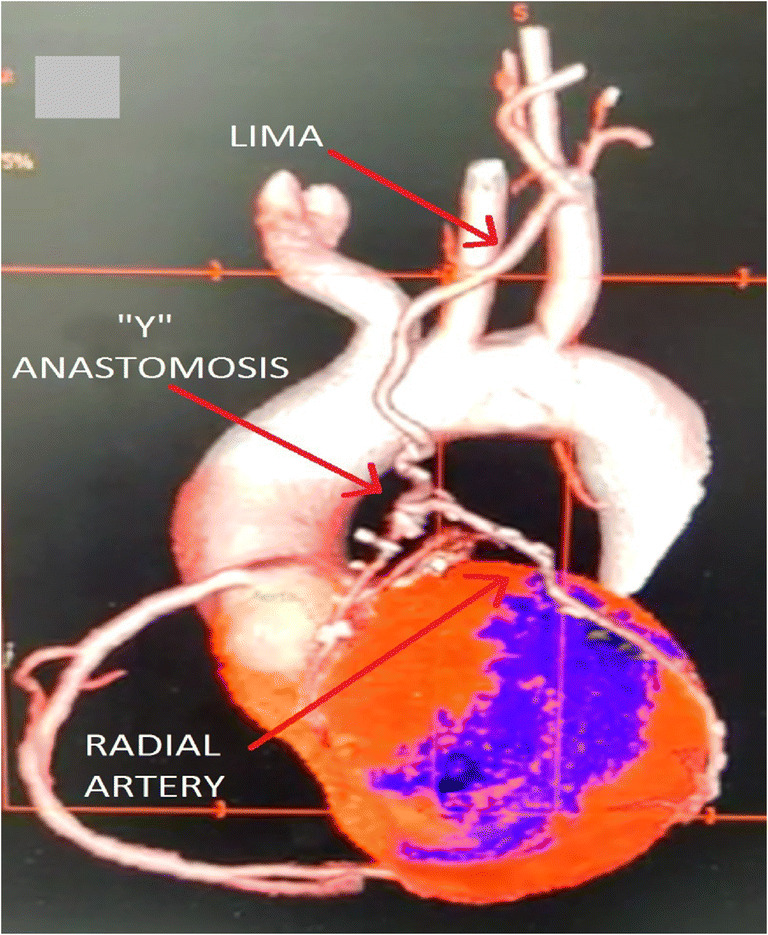
Results: The mean age was 59.33 ± 9.95 (range 37-82) years. The numbers of males and females were 72 and 28 respectively. The preoperative average ejection fraction (EF) was 51.08 ± 9.75%. All these patients underwent CABG via left thoracotomy approach, after satisfying the exclusion criteria. All patients received left internal mammary artery (LIMA) to left anterior descending (LAD) as a standard graft, with the radial artery and saphenous vein being the next alternative conduits. The average length of the incision was 6.06 ± 0.45 cm. Only 2 cases were done on pump. The average number of grafts per patient was 2.33 ± 0.92. The mean operative time was 132.40 ± 11.56 min. The mean duration of ventilation was 4.79 ± 1.90 h and average intensive care unit (ICU) stay was 2.62 ± 0.84 days. There was one conversion and no mortalities in our study. We had analyzed our operative times and noticed a significant reduction after the first 20 cases, which was our learning curve.
Conclusion: MICS CABG can be performed for multivessel disease with the same comfort as for a single or a double vessel disease, once the learning curve has been achieved. Only significant difference from the sternotomy approach was noted in the longer operative times for MICS CABG during the learning curve, and not thereafter. Significant benefits of MICS over sternotomy were noticed in the immediate postoperative parameters like duration of ventilation, mean drainage, postoperative pain, ICU stay, and hospital stay, with no difference in postoperative adverse events.
Keywords: Learning curve; MICS CABG; Multivessel bypass.
© Indian Association of Cardiovascular-Thoracic Surgeons 2020.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflict of interest.
Figures
Comment in
-
MICS CABG: Preoperative and perioperative evaluation.Indian J Thorac Cardiovasc Surg. 2024 Mar;40(2):268-269. doi: 10.1007/s12055-023-01591-8. Epub 2023 Sep 18. Indian J Thorac Cardiovasc Surg. 2024. PMID: 38389774 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources