

Towards Personalized Management of Sarcopenia in COPD
- PMID: 33442246
- PMCID: PMC7800429
- DOI: 10.2147/COPD.S280540
Towards Personalized Management of Sarcopenia in COPD
Abstract
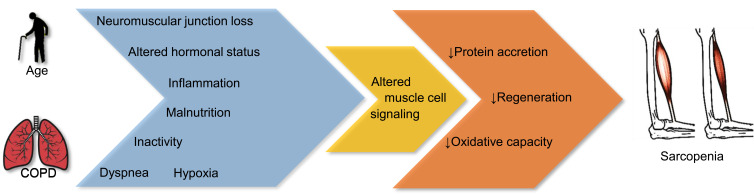
The awareness of the presence and consequences of sarcopenia has significantly increased over the past decade. Sarcopenia is defined as gradual loss of muscle mass and strength and ultimately loss of physical performance associated with aging and chronic disease. The prevalence of sarcopenia is higher in chronic obstructive pulmonary disease (COPD) compared to age-matched controls. Current literature suggests that next to physical inactivity, COPD-specific alterations in physiological processes contribute to accelerated development of sarcopenia. Sarcopenia in COPD can be assessed according to current guidelines, but during physical performance testing, ventilatory limitation should be considered. Treatment of muscle impairment can halt or even reverse sarcopenia, despite respiratory impairment. Exercise training and protein supplementation are currently at the basis of sarcopenia treatment. Furthermore, effective current and new interventions targeting the pulmonary system (eg, smoking cessation, bronchodilators and lung volume reduction surgery) may also facilitate muscle maintenance. Better understanding of disease-specific pathophysiological mechanisms involved in the accelerated development of sarcopenia in COPD will provide new leads to refine nutritional, exercise and physical activity interventions and develop pharmacological co-interventions.
Keywords: anabolics; chronic obstructive pulmonary disease; exercise; nutrition; nutritional assessment; skeletal muscle.
© 2021 van Bakel et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Sarcopenia correlates with systemic inflammation in COPD.Int J Chron Obstruct Pulmon Dis. 2017 Feb 20;12:669-675. doi: 10.2147/COPD.S130790. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 28255238 Free PMC article.
-
Diagnosis, prevalence, and clinical impact of sarcopenia in COPD: a systematic review and meta-analysis.J Cachexia Sarcopenia Muscle. 2020 Oct;11(5):1164-1176. doi: 10.1002/jcsm.12600. Epub 2020 Aug 30. J Cachexia Sarcopenia Muscle. 2020. PMID: 32862514 Free PMC article.
-
Risk Factors of Sarcopenia in COPD Patients: A Meta-Analysis.Int J Chron Obstruct Pulmon Dis. 2024 Jul 9;19:1613-1622. doi: 10.2147/COPD.S456451. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39011123 Free PMC article.
-
Functional tests associated with sarcopenia in moderate chronic obstructive pulmonary disease.Expert Rev Respir Med. 2021 Apr;15(4):569-576. doi: 10.1080/17476348.2021.1850276. Epub 2020 Dec 6. Expert Rev Respir Med. 2021. PMID: 33197358
-
Sarcopenia in chronic obstructive pulmonary disease: A study of prevalence and associated factors in the Southeast Asian population.Chron Respir Dis. 2018 Aug;15(3):250-257. doi: 10.1177/1479972317743759. Epub 2017 Nov 29. Chron Respir Dis. 2018. PMID: 29186972 Free PMC article.
Cited by
-
Influenza A Virus-Driven Airway Inflammation may be Dissociated From Limb Muscle Atrophy in Cigarette Smoke-Exposed Mice.Front Pharmacol. 2022 Mar 18;13:859146. doi: 10.3389/fphar.2022.859146. eCollection 2022. Front Pharmacol. 2022. PMID: 35370652 Free PMC article.
-
Pulmonary Rehabilitation: Mechanisms of Functional Loss and Benefits of Exercise.Respir Care. 2024 May 28;69(6):640-650. doi: 10.4187/respcare.11705. Respir Care. 2024. PMID: 38503465 Free PMC article. Review.
-
Respiratory and Peripheral Muscle Weakness and Body Composition Abnormalities in Non-Cystic Fibrosis Bronchiectasis Patients: Gender Differences.Biomedicines. 2022 Jan 31;10(2):334. doi: 10.3390/biomedicines10020334. Biomedicines. 2022. PMID: 35203543 Free PMC article.
-
Accelerated loss of trunk muscle density and size at L1 vertebral level in male patients with COPD.Front Endocrinol (Lausanne). 2022 Dec 15;13:1087110. doi: 10.3389/fendo.2022.1087110. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36589831 Free PMC article.
-
Association between the Static and Dynamic Lung Function and CT-Derived Thoracic Skeletal Muscle Measurements-A Retrospective Analysis of a 12-Month Observational Follow-Up Pilot Study.Adv Respir Med. 2024 Mar 6;92(2):123-144. doi: 10.3390/arm92020015. Adv Respir Med. 2024. PMID: 38525774 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
