

Surveillance for Hepatocellular Carcinoma Also Improves Survival of Incidentally Detected Intrahepatic Cholangiocarcinoma Arisen in Liver Cirrhosis
- PMID: 33442543
- PMCID: PMC7768136
- DOI: 10.1159/000509059
Surveillance for Hepatocellular Carcinoma Also Improves Survival of Incidentally Detected Intrahepatic Cholangiocarcinoma Arisen in Liver Cirrhosis
Abstract
Background: Due to its poor survival, intrahepatic cholangiocarcinoma (ICC) is held to be a much more aggressive cancer than hepatocellular carcinoma (HCC). In most published series, patients were diagnosed when symptomatic. However, ICC is now increasingly being discovered during the surveillance for HCC in cirrhosis. Whether this earlier detection of ICC is associated with an equally dismal prognosis or not is unknown.
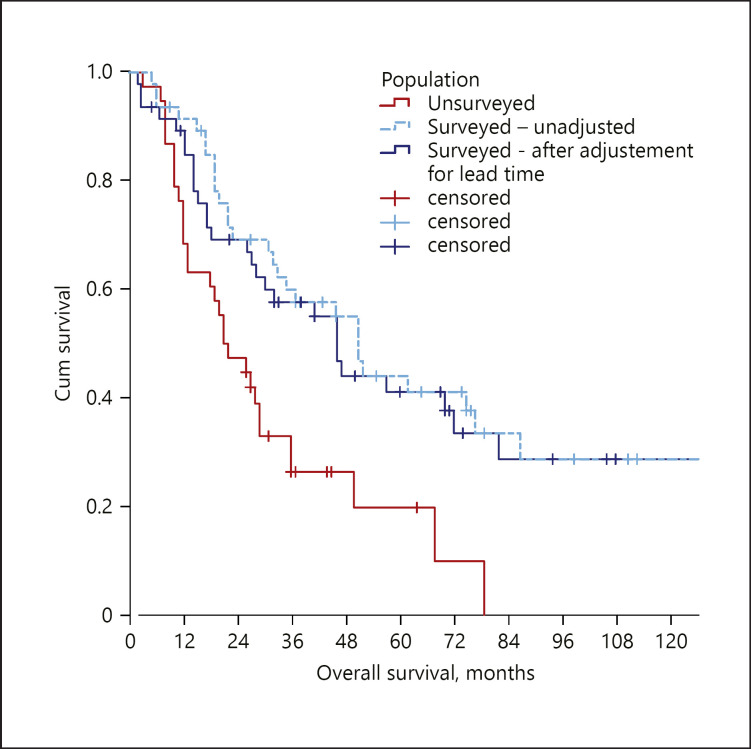
Methods: This is amulticenter retrospective study of consecutive ICC patients. Patients were stratified into subgroups according to the absence/presence of cirrhosis. A propensity score matching was performed to reduce the potential biases. Cirrhotic patients were further stratified according to their surveillance status. The lead-time bias and its potential effects were also estimated.
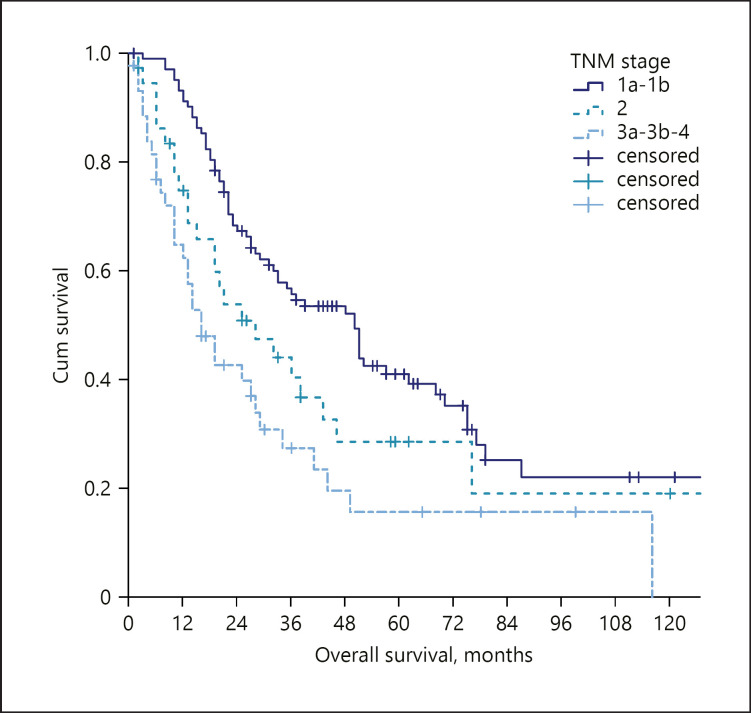
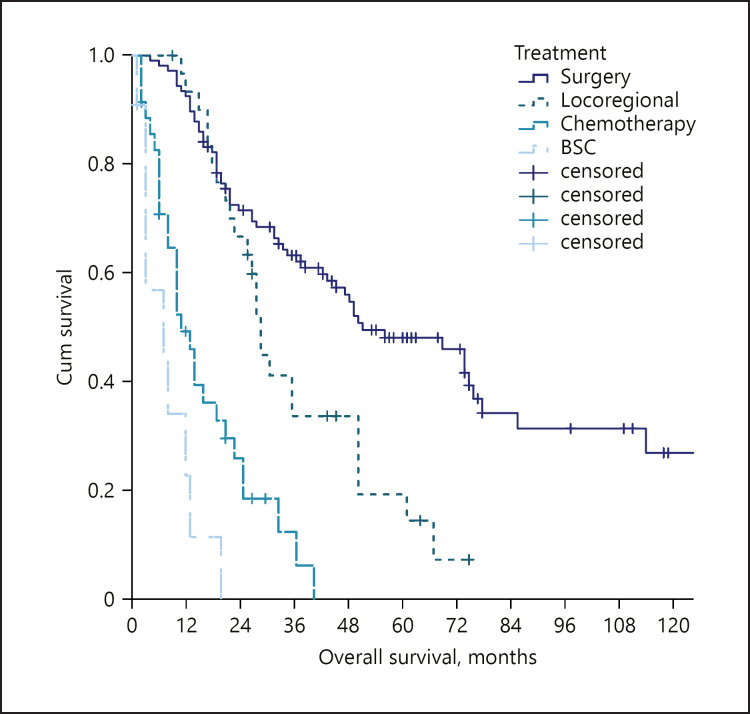
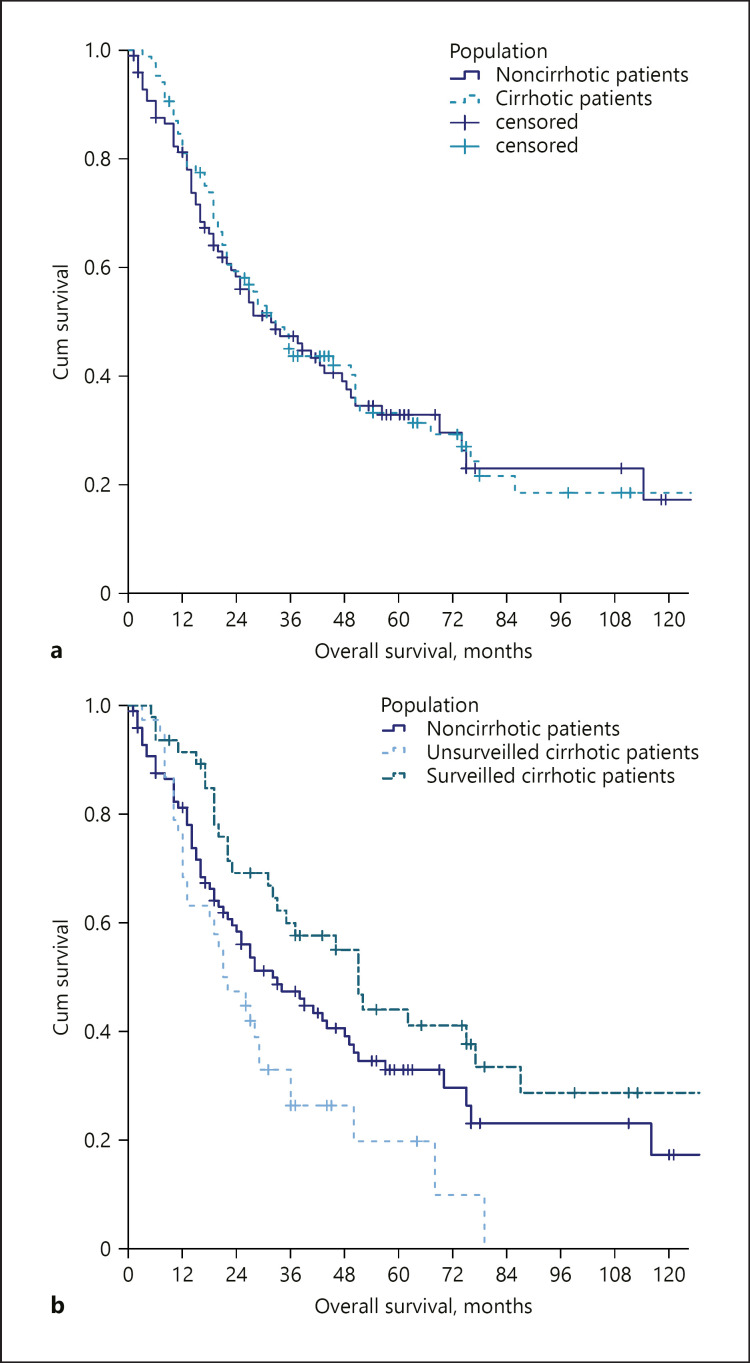
Results: We gathered 184 patients. Eighty-five patients (46.2%) were cirrhotic. Liver cirrhosis was not related to a worse overall survival (33.0 vs. 32.0 months, p = 0.800) even after the propensity score analysis (43.0 in vs. 44.0 months in 54 pairs of patients, p = 0.878). Among the cirrhotic population, 47 (55.3%) patients had received a diagnosis of ICC during a surveillance programme. The 2 subgroups differed in maximum tumour dimensions (30 vs. 48 mm in surveyed and non-surveyed patients, respectively). Surveyed patients were more likely to receive surgical treatments (59.8 vs. 28.9%, p = 0.003). Overall survival was higher in surveyed patients (51.0 vs. 21.0 months, p < 0.001). These benefits were confirmed after correcting for the lead-time bias.
Conclusions: Cirrhotic patients have different clinical presentation and outcomes of ICC according to their surveillance status. In our series, ICC in cirrhosis was not associated with worse OS. Cirrhosis itself should not discourage either surgical or non-surgical treatments.
Keywords: Cholangiocellular carcinoma; Intrahepatic cholangiocarcinoma; Liver cirrhosis; Outcomes; Screening.
Copyright © 2020 by S. Karger AG, Basel.
Conflict of interest statement
Francesco Tovoli: consultant for Bayer AG and advisory board for LaForce; Pietro Guerra: no conflicts to declare; Massimo Iavarone: speaker honoraria from Bayer, Gilead Science, Janssen, BTG, Abbvie, and MSD and consultant for BTG; Letizia Veronese: no conflicts to declare; Matteo Renzulli: no conflicts to declare; Stefania De Lorenzo: no conflicts to declare; Francesca Benevento: no conflicts to declare; Giovanni Brandi: advisory board for Eli-Lilly; Federico Stefanini: no conflicts to declare; Fabio Piscaglia: consultant for Astrazeneca, Bayer AG, EISAI, GE, and Tiziana life sciences; speaker's bureau honoraria from Bayer AG, Bracco, EISAI, and Laforce; and research contract with Esaote.
Figures
References
-
- Li YY, Li H, Lv P, Liu G, Li XR, Tian BN, et al. Prognostic value of cirrhosis for intrahepatic cholangiocarcinoma after surgical treatment. J Gastrointest Surg. 2011;15((4)):608–13. - PubMed
-
- Luo X, Yuan L, Wang Y, Ge R, Sun Y, Wei G. Survival outcomes and prognostic factors of surgical therapy for all potentially resectable intrahepatic cholangiocarcinoma: a large single-center cohort study. J Gastrointest Surg. 2014;18((3)):562–72. - PubMed
-
- Jesper D, Heyn SG, Schellhaas B, Pfeifer L, Goertz RS, Zopf S, et al. Effects of liver cirrhosis and patient condition on clinical outcomes in intrahepatic cholangiocarcinoma: a retrospective analysis of 156 cases in a single center. Eur J Gastroenterol Hepatol. 2018;30((5)):552–6. - PubMed
-
- Forner A, Vidili G, Rengo M, Bujanda L, Ponz‐Sarvisé M, Lamarca A. Clinical presentation, diagnosis and staging of cholangiocarcinoma. Liver Int. 2019;39((Suppl 1)):98–107. - PubMed
LinkOut - more resources
Full Text Sources
