

Novel Strategy of Curettage and Adjuvant Microwave Therapy for the Treatment of Giant Cell Tumor of Bone in Extremities: A Preliminary Study
- PMID: 33442922
- PMCID: PMC7862174
- DOI: 10.1111/os.12865
Novel Strategy of Curettage and Adjuvant Microwave Therapy for the Treatment of Giant Cell Tumor of Bone in Extremities: A Preliminary Study
Abstract
Objectives: To evaluate whether curettage with adjuvant microwave therapy was successful in the treatment of giant cell tumor of the bone (GCTB) in extremities, especially for GCTB with pathological fractures and GCTB of the distal radius.
Methods: This was a retrospective study of 54 cases of GCTB of the extremities treated by curettage with adjuvant microwave therapy between 2007 and 2019. Five patients were lost to follow up and excluded from the study. A total of 33 male and 21 female patients were included in this study. Patients were aged 15-57 years (mean 29.72 ± 10.48 years). Among these patients, there were 10 cases of GCTB with pathological fractures and eight cases of GCTB of the distal radius; one of these cases was combined with a pathological fracture. Comprehensive imaging examinations (X-rays [including lesion site and chest], CT, MRI, emission computed tomography, and pathology examination) of all patients were reviewed. The clinical staging of these patients were evaluated radiologically using the Campanacci classification system based on the extent of spread of the tumor. All patients underwent curettage with adjuvant microwave therapy. Clinical and imaging evaluations were performed in all cases to check for recurrence or metastasis. Lower limb and upper limber function were assessed using the Musculoskeletal Tumor Society score (MSTS), and wrist function was assessed according to the disabilities of the arm, shoulder and hand (DASH) score. Data on surgical-related complications were recorded.
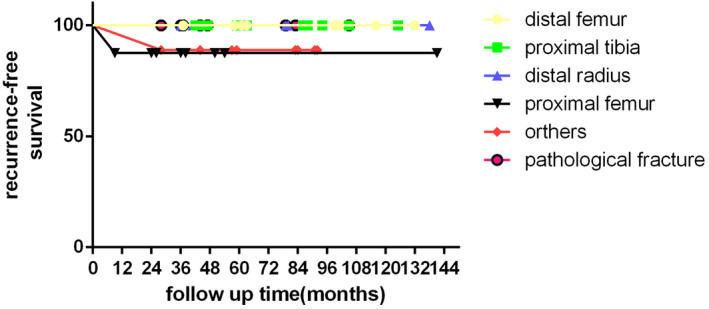
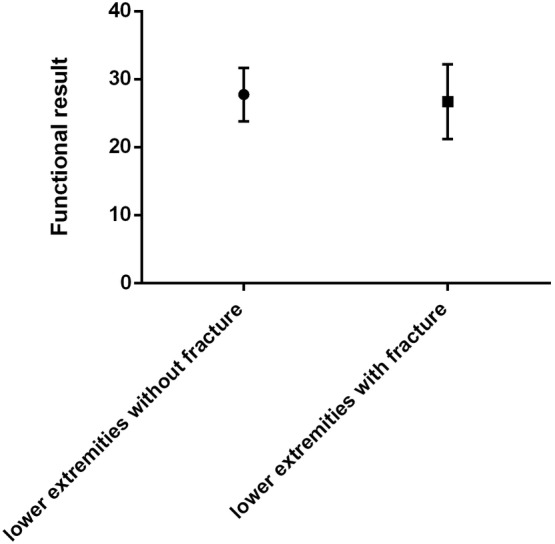
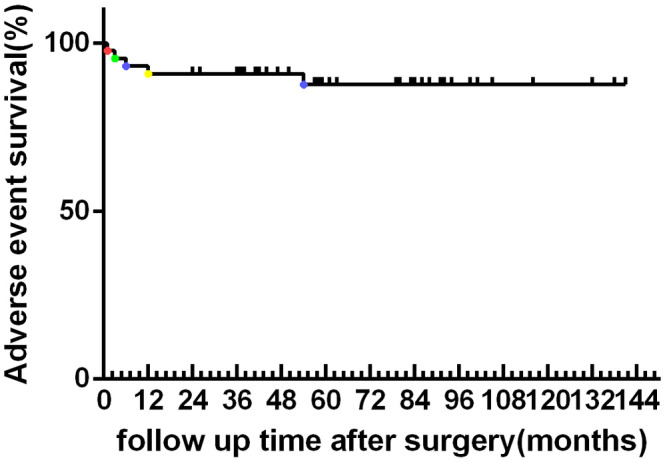
Results: All cases were followed up for 24-126 months (mean 60.69 ± 29.61 months). There were 24 patients with a Campanacci grade of 3 and 30 with a Campanacci grade of 2. The 52 patients were continuously disease-free. The local recurrence rate was 3.70% (2 patients). One patient had recurrence in the proximal femur, and the other developed in soft tissue of the calf muscle. No recurrence occurred for GCTB of the distal radius. One recurrence occurred in a GCTB with pathological fractures. The intervals were 9 and 28 months, respectively. The cases of recurrence all had a Campanacci grade of 3 (8.33%). The median MSTS among the 54 patients was 27.67 ± 3.81. The mean wrist function DASH score was 8.30 ± 2.53. The mean MSTS was 28.67 ± 1.63 and 26.71 ± 5.49 for patients with GCTB of the distal radius and for those with pathological fractures, respectively. In comparing patients with and without pathological fractures, there was no significant difference in the MSTS functional score. Five patients had complications after the surgery.
Conclusion: Curettage with adjuvant microwave ablation therapy provided favorable local control and satisfactory functional outcomes in the treatment of GCTB, especially for cases with pathological fractures and those with GCTB of the distal radius.
Keywords: Distal radius; Giant cell tumor; Microwave ablation; Pathological fracture.
© 2020 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures
Similar articles
-
Preoperative denosumab combined with microwave ablation for joint preservation in advanced giant cell tumor of bone: a retrospective study.J Orthop Surg Res. 2025 Feb 18;20(1):174. doi: 10.1186/s13018-025-05589-3. J Orthop Surg Res. 2025. PMID: 39966973 Free PMC article.
-
Combined preoperative denosumab and adjuvant microwave ablation for high-risk giant cell tumor of bone: a retrospective study in a single center.J Orthop Surg Res. 2024 Aug 17;19(1):488. doi: 10.1186/s13018-024-04981-9. J Orthop Surg Res. 2024. PMID: 39154187 Free PMC article.
-
Denosumab combined with en bloc resection and arthrodesis for recurrent grade 3 giant cell tumor of bone in distal radius.J Orthop Surg Res. 2024 Sep 28;19(1):607. doi: 10.1186/s13018-024-05092-1. J Orthop Surg Res. 2024. PMID: 39342379 Free PMC article.
-
Present day controversies and consensus in curettage for giant cell tumor of bone.J Clin Orthop Trauma. 2019 Nov-Dec;10(6):1015-1020. doi: 10.1016/j.jcot.2019.09.017. Epub 2019 Oct 11. J Clin Orthop Trauma. 2019. PMID: 31736607 Free PMC article. Review.
-
Current Concepts in the Treatment of Giant Cell Tumor of Bone: An Update.Curr Oncol. 2024 Apr 8;31(4):2112-2132. doi: 10.3390/curroncol31040157. Curr Oncol. 2024. PMID: 38668060 Free PMC article. Review.
Cited by
-
Stereotactic body radiotherapy for lung metastases in a patient with giant cell tumor of bone: a case report and literature review.Ann Transl Med. 2022 Feb;10(3):156. doi: 10.21037/atm-21-6575. Ann Transl Med. 2022. PMID: 35284555 Free PMC article.
-
Conservative surgery with microwave ablation for recurrent bone tumor in the extremities: a single-center study.BMC Cancer. 2022 Nov 2;22(1):1122. doi: 10.1186/s12885-022-10233-y. BMC Cancer. 2022. PMID: 36320002 Free PMC article.
-
Microwave in situ inactivation in the treatment of bone giant cell tumor: a mid-term descriptive study.J Cancer Res Clin Oncol. 2023 Jul;149(8):4653-4661. doi: 10.1007/s00432-022-04348-9. Epub 2022 Oct 3. J Cancer Res Clin Oncol. 2023. PMID: 36190550 Free PMC article.
-
Denosumab combined with microwave ablation excisional scraping for giant cell tumor of the thoracic spine: a case report and literature review.Front Oncol. 2024 Sep 19;14:1402550. doi: 10.3389/fonc.2024.1402550. eCollection 2024. Front Oncol. 2024. PMID: 39364313 Free PMC article.
-
Giant cell tumor of bone and secondary osteoarthritis.Heliyon. 2024 May 9;10(10):e30890. doi: 10.1016/j.heliyon.2024.e30890. eCollection 2024 May 30. Heliyon. 2024. PMID: 38807896 Free PMC article. Review.
References
-
- Cheng DD, Hu T, Zhang HZ, Huang J, Yang QC. Factors affecting the recurrence of giant cell tumor of bone after surgery: a clinicopathological study of 80 cases from a single center. Cell Physiol Biochem, 2015, 36: 1961–1970. - PubMed
-
- Campanacci M, Baldini N, Boriani S, Sudanese A. Giant‐cell tumor of bone. J Bone Joint Surg Am, 1987, 69: 106–114. - PubMed
-
- Ghert MA, Rizzo M, Harrelson JM, Scully SP. Giant‐cell tumor of the appendicular skeleton. Clin Orthop Relat Res, 2002, 400: 201–210. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
