

Parent and Physician Understanding of Prognosis in Hospitalized Children With Advanced Heart Disease
- PMID: 33442989
- PMCID: PMC7955315
- DOI: 10.1161/JAHA.120.018488
Parent and Physician Understanding of Prognosis in Hospitalized Children With Advanced Heart Disease
Abstract
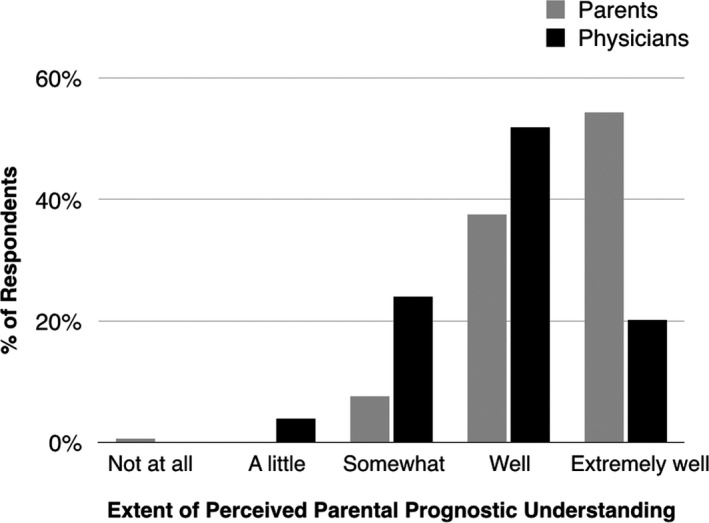
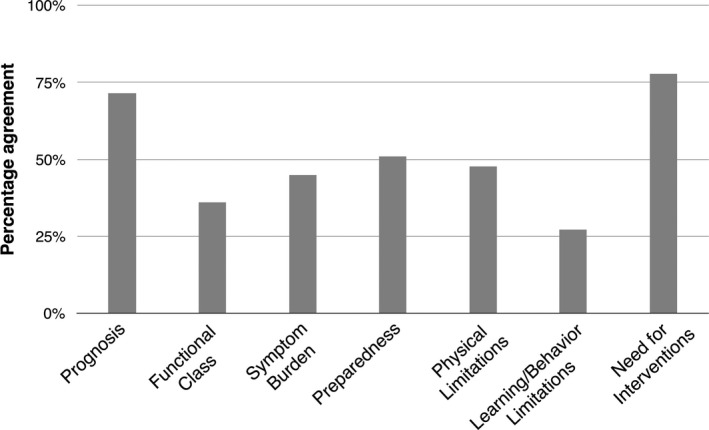
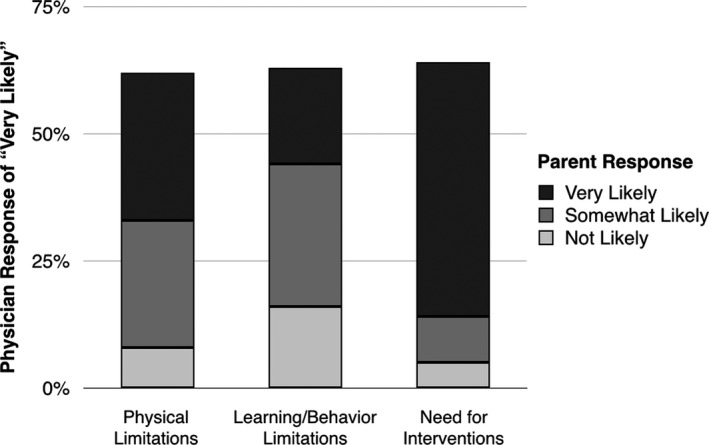
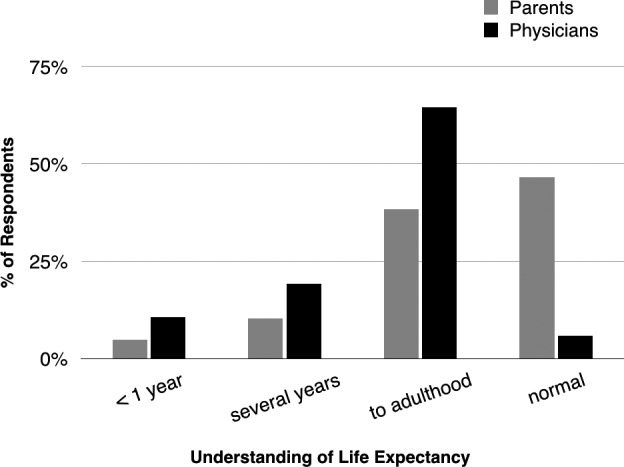
Background The unpredictable trajectory of pediatric advanced heart disease makes prognostication difficult for physicians and informed decision-making challenging for families. This study evaluated parent and physician understanding of disease burden and prognosis in hospitalized children with advanced heart disease. Methods and Results A longitudinal survey study of parents and physicians caring for patients with advanced heart disease age 30 days to 19 years admitted for ≥7 days was performed over a 1-year period (n=160 pairs). Percentage agreement and weighted kappa statistics were used to assess agreement. Median patient age was 1 year (interquartile range, 1-5), 39% had single-ventricle lesions, and 37% were in the cardiac intensive care unit. Although 92% of parents reported understanding their child's prognosis "extremely well" or "well," 28% of physicians thought parents understood the prognosis only "a little," "somewhat," or "not at all." Better parent-reported prognostic understanding was associated with greater preparedness for their child's medical problems (odds ratio, 4.7; 95% CI, 1.4-21.7, P=0.02). There was poor parent-physician agreement in assessing functional class, symptom burden, and likelihood of limitations in physical activity and learning/behavior; on average, parents were more optimistic. Many parents (47%) but few physicians (6%) expected the child to have normal life expectancy. Conclusions Parents and physicians caring for children with advanced heart disease differed in their perspectives regarding prognosis and disease burden. Physicians tended to underestimate the degree of parent-reported symptom burden. Parents were less likely to expect limitations in physical activity, learning/behavior, and life expectancy. Combined interventions involving patient-reported outcomes, parent education, and physician communication tools may be beneficial.
Keywords: communication; congenital heart disease; heart failure; pediatrics; prognosis; quality of life.
Conflict of interest statement
None.
Figures
Similar articles
-
Parent-Provider Communication in Hospitalized Children with Advanced Heart Disease.Pediatr Cardiol. 2022 Dec;43(8):1761-1769. doi: 10.1007/s00246-022-02913-0. Epub 2022 May 10. Pediatr Cardiol. 2022. PMID: 35538320
-
Physician and parent perceptions of prognosis and end-of-life experience in children with advanced heart disease.J Palliat Med. 2015 Apr;18(4):318-23. doi: 10.1089/jpm.2014.0305. Epub 2014 Dec 10. J Palliat Med. 2015. PMID: 25493354
-
The experience of fathers of children hospitalised with advanced heart disease.Cardiol Young. 2024 Jun;34(6):1274-1278. doi: 10.1017/S1047951123004390. Epub 2024 Jan 10. Cardiol Young. 2024. PMID: 38196389
-
Understanding Parental Preferences for Participants in Medical Decision-making for Their Hospitalized Children.Hosp Pediatr. 2018 Apr;8(4):200-206. doi: 10.1542/hpeds.2017-0008. Epub 2018 Mar 7. Hosp Pediatr. 2018. PMID: 29514853 Review.
-
An integrative review of communication between parents and nurses of hospitalized technology-dependent children.Worldviews Evid Based Nurs. 2014 Dec;11(6):369-75. doi: 10.1111/wvn.12065. Epub 2014 Sep 17. Worldviews Evid Based Nurs. 2014. PMID: 25230724 Review.
Cited by
-
Medical and End-of-Life Decision-Making Preferences in Adolescents and Young Adults with Advanced Heart Disease and Their Parents.JAMA Netw Open. 2023 May 1;6(5):e2311957. doi: 10.1001/jamanetworkopen.2023.11957. JAMA Netw Open. 2023. PMID: 37145598 Free PMC article.
-
Palliative Care Education in Pediatric Cardiology Fellowships: A Survey of Program Directors.Pediatr Cardiol. 2025 Jun 22. doi: 10.1007/s00246-025-03926-1. Online ahead of print. Pediatr Cardiol. 2025. PMID: 40544233
-
Parent and healthcare professional experiences of critical congenital heart disease in New Zealand to advance health equity.BMC Health Serv Res. 2024 Aug 26;24(1):991. doi: 10.1186/s12913-024-11410-4. BMC Health Serv Res. 2024. PMID: 39187808 Free PMC article.
-
Palliative Care in Children With Advanced Heart Disease in a Tertiary Care Environment: A Mini Review.Front Cardiovasc Med. 2022 Apr 8;9:863031. doi: 10.3389/fcvm.2022.863031. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35463792 Free PMC article. Review.
-
Parent-Provider Communication in Hospitalized Children with Advanced Heart Disease.Pediatr Cardiol. 2022 Dec;43(8):1761-1769. doi: 10.1007/s00246-022-02913-0. Epub 2022 May 10. Pediatr Cardiol. 2022. PMID: 35538320
References
-
- Rossano JW, Kim JJ, Decker JA, Price JF, Zafar F, Graves DE, Morales DLS, Heinle JS, Bozkurt B, Towbin JA, et al. Prevalence, morbidity, and mortality of heart failure‐related hospitalizations in children in the United States: a population‐based study. J Card Fail. 2012;18:459–470. - PubMed
-
- Morell E, Moynihan K, Wolfe J, Blume ED. Palliative care and paediatric cardiology: current evidence and future directions. Lancet Child Adolesc Health. 2019;3:502–510. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
