

Racial Differences in AKI Incidence Following Percutaneous Coronary Intervention
- PMID: 33443096
- PMCID: PMC7920184
- DOI: 10.1681/ASN.2020040502
Racial Differences in AKI Incidence Following Percutaneous Coronary Intervention
Abstract
Background: Undergoing percutaneous coronary intervention (PCI) is a risk factor for AKI development, but few studies have quantified racial differences in AKI incidence after this procedure.
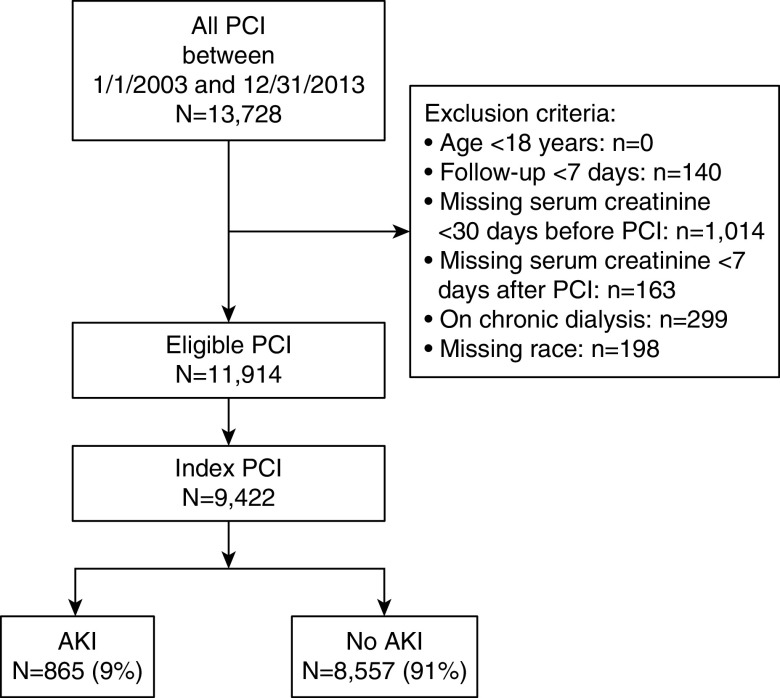
Methods: We examined the association of self-reported race (Black, White, or other) and baseline eGFR with AKI incidence among patients who underwent PCI at Duke University Medical Center between January 1, 2003, and December 31, 2013. We defined AKI as a 0.3 mg/dl absolute increase in serum creatinine within 48 hours, or ≥1.5-fold relative elevation within 7 days post-PCI from the reference value ascertained within 30 days before PCI.
Results: Of 9422 patients in the analytic cohort (median age 63 years; 33% female; 75% White, 20% Black, 5% other race), 9% developed AKI overall (14% of Black, 8% of White, 10% of others). After adjustment for demographics, socioeconomic status, comorbidities, predisposing medications, PCI indication, periprocedural AKI prophylaxis, and PCI procedural characteristics, Black race was associated with increased odds for incident AKI compared with White race (odds ratio [OR], 1.79; 95% confidence interval [95% CI], 1.48 to 2.15). Compared with Whites, odds for incident AKI were not significantly higher in other patients (OR, 1.30; 95% CI, 0.93 to 1.83). Low baseline eGFR was associated with graded, higher odds of AKI incidence (P value for trend <0.001); however, there was no interaction between race and baseline eGFR on odds for incident AKI (P value for interaction = 0.75).
Conclusions: Black patients had greater odds of developing AKI after PCI compared with White patients. Future investigations should identify factors, including multiple domains of social determinants, that predispose Black individuals to disparate AKI risk after PCI.
Keywords: African Americans; acute kidney injury; percutaneous coronary intervention; racial disparities.
Copyright © 2021 by the American Society of Nephrology.
Figures
References
-
- Rewa O, Bagshaw SM: Acute kidney injury-epidemiology, outcomes and economics. Nat Rev Nephrol 10: 193–207, 2014 - PubMed
-
- Hoste EA, Schurgers M: Epidemiology of acute kidney injury: How big is the problem? Crit Care Med 36[Suppl]: S146–S151, 2008 - PubMed
-
- Grams ME, Matsushita K, Sang Y, Estrella MM, Foster MC, Tin A, et al. .: Explaining the racial difference in AKI incidence. J Am Soc Nephrol 25: 1834–1841, 2014 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
