

Manipulation of ACE2 expression in COVID-19
- PMID: 33443121
- PMCID: PMC7757413
- DOI: 10.1136/openhrt-2020-001424
Manipulation of ACE2 expression in COVID-19
Abstract
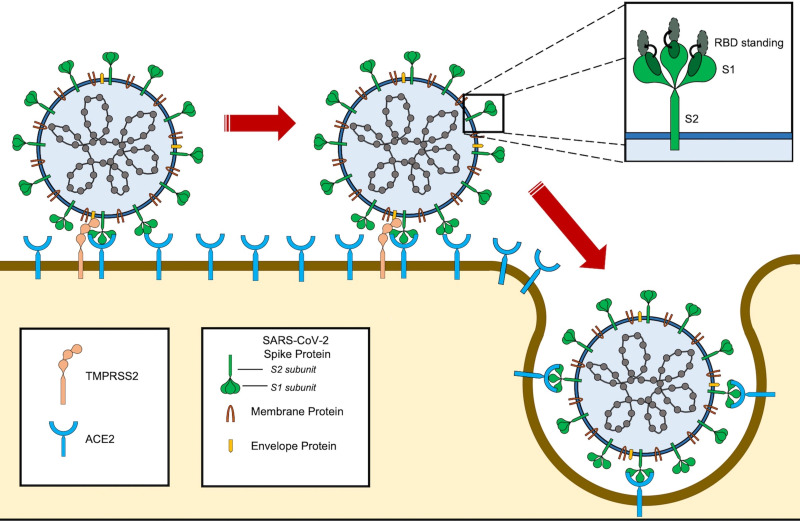
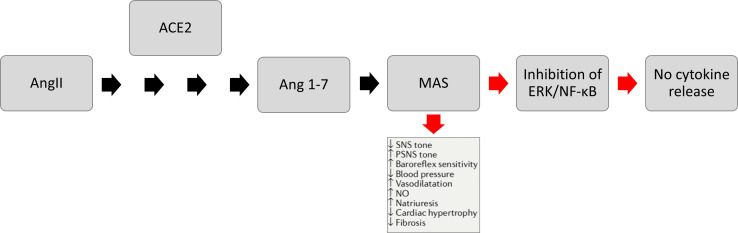
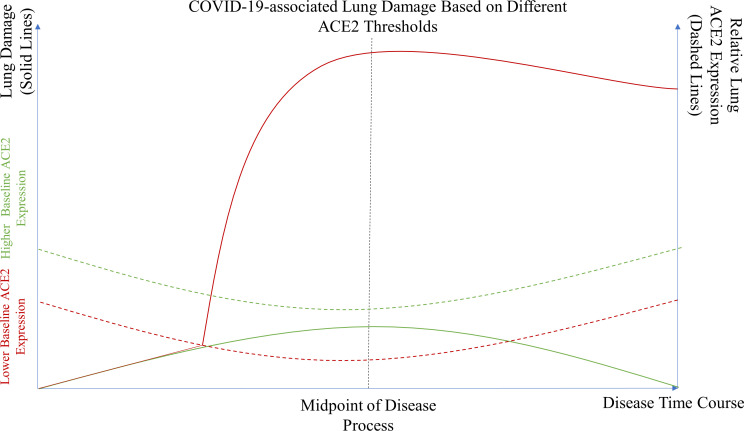
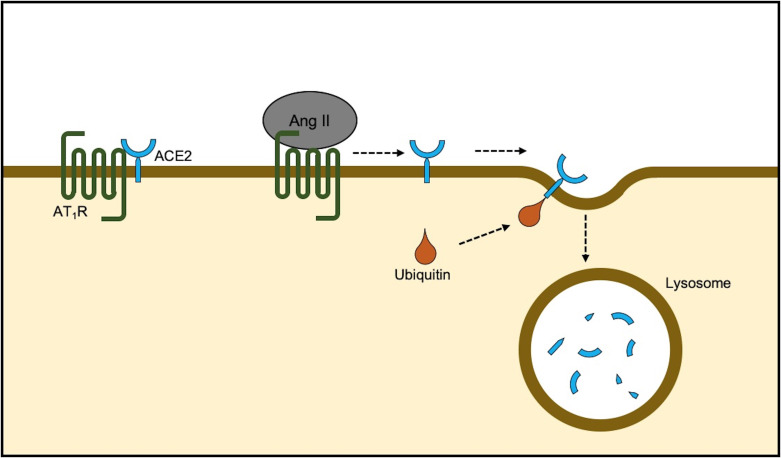
SARS-CoV-2 is the virus responsible for the ongoing COVID-19 outbreak. The virus uses ACE2 receptor for viral entry. ACE2 is part of the counter-regulatory renin-angiotensin-aldosterone system and is also expressed in the lower respiratory tract along the alveolar epithelium. There is, however, significant controversy regarding the role of ACE2 expression in COVID-19 pathogenesis. Some have argued that decreasing ACE2 expression would result in decreased susceptibility to the virus by decreasing available binding sites for SARS-CoV-2 and restricting viral entry into the cells. Others have argued that, like the pathogenesis of other viral pneumonias, including those stemming from previous severe acute respiratory syndrome (SARS) viruses, once SARS-CoV-2 binds to ACE2, it downregulates ACE2 expression. Lack of the favourable effects of ACE2 might exaggerate lung injury by a variety of mechanisms. In order to help address this controversy, we conducted a literature search and review of relevant preclinical and clinical publications pertaining to SARS-CoV-2, COVID-19, ACE2, viral pneumonia, SARS, acute respiratory distress syndrome and lung injury. Our review suggests, although controversial, that patients at increased susceptibility to COVID-19 complications may have reduced baseline ACE2, and by modulating ACE2 expression one can possibly improve COVID-19 outcomes. Herein, we elucidate why and how this potential mechanism might work.
Keywords: hypertension; intensive care; lung injury.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous