

Effectiveness of Sequential Chemoradiation vs Concurrent Chemoradiation or Radiation Alone in Adjuvant Treatment After Hysterectomy for Cervical Cancer: The STARS Phase 3 Randomized Clinical Trial
- PMID: 33443541
- PMCID: PMC7809615
- DOI: 10.1001/jamaoncol.2020.7168
Effectiveness of Sequential Chemoradiation vs Concurrent Chemoradiation or Radiation Alone in Adjuvant Treatment After Hysterectomy for Cervical Cancer: The STARS Phase 3 Randomized Clinical Trial
Abstract
Importance: There is no current consensus on the role of chemotherapy in addition to radiation for postoperative adjuvant treatment of patients with early-stage cervical cancer with adverse pathological factors.
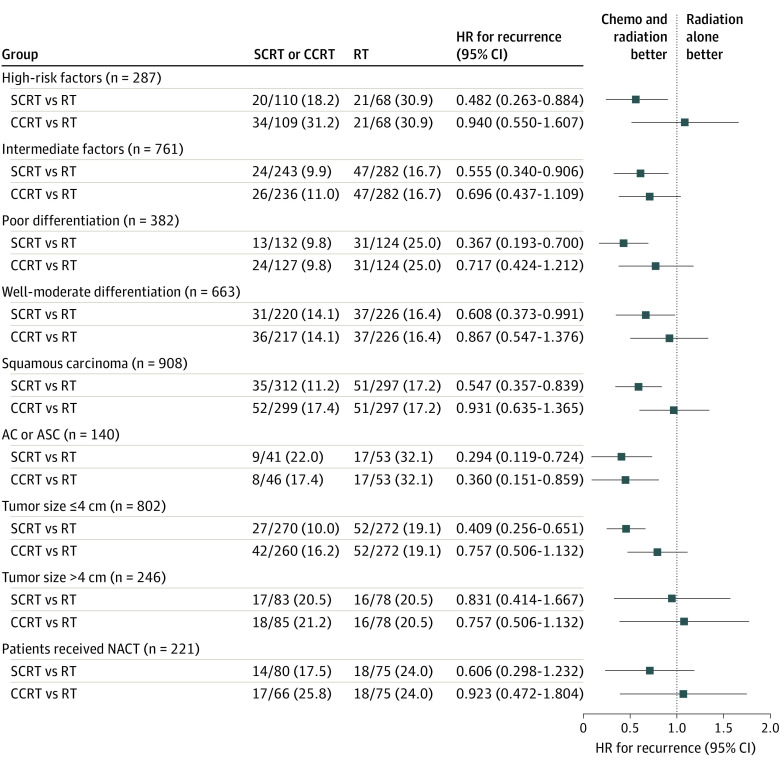
Objective: To evaluate the clinical benefits of sequential chemoradiation (SCRT) and concurrent chemoradiation (CCRT) compared with radiation alone (RT) as a postoperative adjuvant treatment in early-stage cervical cancer.
Design, setting, and participants: After radical hysterectomy at 1 of 8 participating hospitals in China, patients with FIGO (International Federation of Gynecology and Obstetrics) stage IB to IIA cervical cancer with adverse pathological factors were randomized 1:1:1 to receive adjuvant RT, CCRT, or SCRT. Data were collected from February 2008 to December 2018.
Interventions: Patients received adjuvant RT (total dose, 45-50 Gy), CCRT (weekly cisplatin, 30-40 mg/m2), or SCRT (cisplatin, 60-75 mg/m2, plus paclitaxel, 135-175 mg/m2) in a 21-day cycle, given 2 cycles before and 2 cycles after radiotherapy, respectively.
Main outcomes and measures: The primary end point was the rate of disease-free survival (DFS) at 3 years.
Results: A total of 1048 women (median [range] age, 48 [23-65] years) were included in the analysis (350 in the RT group, 345 in the CCRT group, and 353 in the SCRT group). Baseline demographic and disease characteristics were balanced among the treatment groups except that the rate of lymph node involvement was lowest in the RT group (18.3%). In the intention-to-treat population, SCRT was associated with a higher rate of DFS than RT (3-year rate, 90.0% vs 82.0%; hazard ratio [HR], 0.52; 95% CI, 0.35-0.76) and CCRT (90.0% vs 85.0%; HR, 0.65; 95% CI, 0.44-0.96). Treatment with SCRT also decreased cancer death risk compared with RT (5-year rate, 92.0% vs 88.0%; HR, 0.58; 95% CI, 0.35-0.95) after adjustment for lymph node involvement. However, neither DFS nor cancer death risk was different among patients treated with CCRT or RT.
Conclusions and relevance: In this randomized clinical trial, conducted in a postoperative adjuvant treatment setting, SCRT, rather than CCRT, resulted in a higher DFS and lower risk of cancer death than RT among women with early-stage cervical cancer.
Trial registration: ClinicalTrials.gov Identifier: NCT00806117.
Conflict of interest statement
Figures


Comment in
-
Sequential Chemotherapy for Early-Stage, Post-Radical Hysterectomy Cervical Cancer: Are the STARS Aligned?JAMA Oncol. 2021 Mar 1;7(3):353-354. doi: 10.1001/jamaoncol.2020.7184. JAMA Oncol. 2021. PMID: 33443572 No abstract available.
-
SCRT for early stage cervical cancer.Nat Rev Clin Oncol. 2021 Mar;18(3):132. doi: 10.1038/s41571-021-00480-6. Nat Rev Clin Oncol. 2021. PMID: 33514912 No abstract available.
-
[Effectiveness of sequential vs concurrent chemoradiation or radiation alone in the adjuvant treatment of cervical cancer after hysterectomy].Strahlenther Onkol. 2021 Aug;197(8):746-748. doi: 10.1007/s00066-021-01796-z. Epub 2021 May 30. Strahlenther Onkol. 2021. PMID: 34052853 Free PMC article. German. No abstract available.
-
Sequential Chemoradiotherapy vs Concurrent Chemoradiotherapy or Radiotherapy Alone in Adjuvant Treatment for Patients With Cervical Cancer.JAMA Oncol. 2021 Sep 1;7(9):1404. doi: 10.1001/jamaoncol.2021.2110. JAMA Oncol. 2021. PMID: 34264280 No abstract available.
-
Sequential Chemoradiotherapy vs Concurrent Chemoradiotherapy or Radiotherapy Alone in Adjuvant Treatment for Patients With Cervical Cancer-Reply.JAMA Oncol. 2021 Sep 1;7(9):1404-1405. doi: 10.1001/jamaoncol.2021.2113. JAMA Oncol. 2021. PMID: 34264307 No abstract available.
References
-
- Monk BJ, Wang J, Im S, et al. ; Gynecologic Oncology Group; Southwest Oncology Group; Radiation Therapy Oncology Group . Rethinking the use of radiation and chemotherapy after radical hysterectomy: a clinical-pathologic analysis of a Gynecologic Oncology Group/Southwest Oncology Group/Radiation Therapy Oncology Group trial. Gynecol Oncol. 2005;96(3):721-728. doi: 10.1016/j.ygyno.2004.11.007 - DOI - PubMed
-
- Peters WA III, Liu PY, Barrett RJ II, et al. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J Clin Oncol. 2000;18(8):1606-1613. doi: 10.1200/JCO.2000.18.8.1606 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
