

Effects of Community-based Exercise Prehabilitation for Patients Scheduled for Colorectal Surgery With High Risk for Postoperative Complications: Results of a Randomized Clinical Trial
- PMID: 33443905
- PMCID: PMC8746915
- DOI: 10.1097/SLA.0000000000004702
Effects of Community-based Exercise Prehabilitation for Patients Scheduled for Colorectal Surgery With High Risk for Postoperative Complications: Results of a Randomized Clinical Trial
Abstract
Objective: To assess the effects of a 3-week community-based exercise program on 30-day postoperative complications in high-risk patients scheduled for elective colorectal resection for (pre)malignancy.
Summary background data: Patients with a low preoperative aerobic fitness undergoing colorectal surgery have an increased risk of postoperative complications. It remains, however, to be demonstrated whether prehabilitation in these patients reduces postoperative complications.
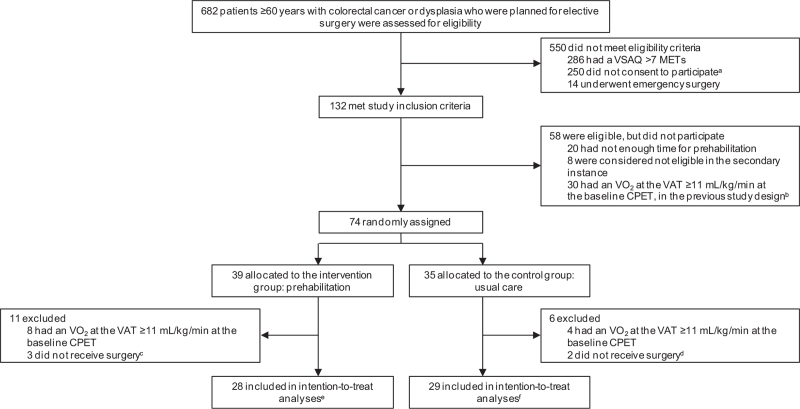
Methods: This 2-center, prospective, single-blinded randomized clinical trial was carried out in 2 large teaching hospitals in the Netherlands. Patients (≥60 years) with colorectal (pre)malignancy scheduled for elective colorectal resection and with a score ≤7 metabolic equivalents on the veterans-specific activity questionnaire were randomly assigned to the prehabilitation group or the usual care group by using block-stratified randomization. An oxygen uptake at the ventilatory anaerobic threshold <11 mL/kg/min at the baseline cardiopulmonary exercise test was the final inclusion criterion. Inclusion was based on a power analysis. Patients in the prehabilitation group participated in a personalized 3-week (3 sessions per week, nine sessions in total) supervised exercise program given in community physical therapy practices before colorectal resection. Patients in the reference group received usual care. The primary outcome was the number of patients with one or more complications within 30 days of surgery, graded according to the Clavien-Dindo classification. Data were analyzed on an intention-to-treat basis.
Results: Between February 2014 and December 2018, 57 patients [30 males and 27 females; mean age 73.6 years (standard deviation 6.1), range 61-88 years] were randomized to either prehabilitation (n = 28) or usual care (n = 29). The rate of postoperative complications was lower in the prehabilitation group (n = 12, 42.9%) than in the usual care group (n = 21, 72.4%, relative risk 0.59, 95% confidence interval 0.37-0.96, P = 0.024).
Conclusions: Exercise prehabilitation reduced postoperative complications in high-risk patients scheduled to undergo elective colon resection for (pre)malignancy. Prehabilitation should be considered as usual care in high-risk patients scheduled for elective colon, and probably also rectal, surgery.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
JMK received research funding from Amgen. Amgen had no role in the study design, acquisition, analysis, and/or interpretation of the data, nor in writing the report and submission. Other authors report no conflicts of interest.
Figures
Comment in
-
Comment on "Effects of Community-based Exercise Prehabilitation for Patients Scheduled for Colorectal Surgery With High Risk for Postoperative Complications: Results of a Randomized Clinical Trial".Ann Surg. 2021 Dec 1;274(6):e931-e932. doi: 10.1097/SLA.0000000000005094. Ann Surg. 2021. PMID: 34784679 No abstract available.
-
Comment on: "Effects of Community-based Exercise Prehabilitation for Patients Scheduled for Colorectal Surgery with High Risk for Postoperative Complications: Results of a Randomized Clinical Trial".Ann Surg. 2022 Dec 1;276(6):e1120. doi: 10.1097/SLA.0000000000005288. Epub 2021 Nov 9. Ann Surg. 2022. PMID: 35129501 No abstract available.
-
Response to the Comments of Onerup et al and Lu and Song on: "Effects of Community-based Exercise Prehabilitation for Patients Scheduled for Colorectal Surgery With High Risk for Postoperative Complications: Results of a Randomized Clinical Trial".Ann Surg. 2022 Dec 1;276(6):e1126-e1128. doi: 10.1097/SLA.0000000000005474. Epub 2022 Jul 7. Ann Surg. 2022. PMID: 35797607 No abstract available.
References
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394–424. - PubMed
-
- Dutch institute for clinical auditing (DICA) Leiden. DICA jaarrapportage 2018: Dutch ColoRectal Audit (DCRA). Available at: https://dica.nl/jaarrapportage-2018/dcra. Accessed April 20, 2020.
-
- Govaert JA, Fiocco M, van Dijk WA, et al. Costs of complications after colorectal cancer surgery in the Netherlands: building the business case for hospitals. Eur J Surg Oncol 2015; 41:1059–1067. - PubMed
-
- Moran J, Guinan E, McCormick P, et al. The ability of prehabilitation to influence postoperative outcome after intra-abdominal operation: A systematic review and meta-analysis. Surgery 2016; 160:1189–1201. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
