

Neurofibromatosis Type 2 (NF2) and the Implications for Vestibular Schwannoma and Meningioma Pathogenesis
- PMID: 33445724
- PMCID: PMC7828193
- DOI: 10.3390/ijms22020690
Neurofibromatosis Type 2 (NF2) and the Implications for Vestibular Schwannoma and Meningioma Pathogenesis
Abstract
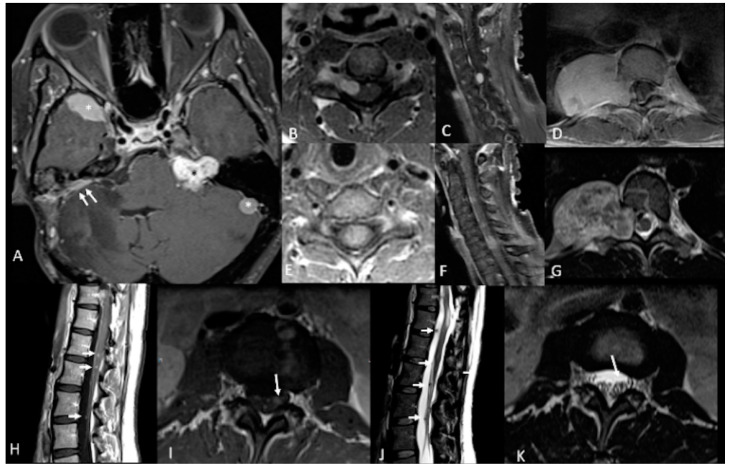
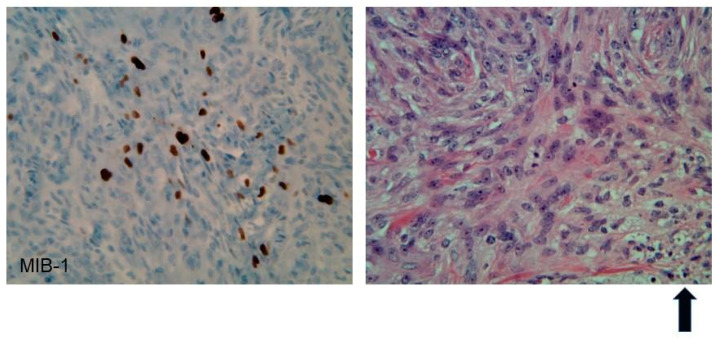
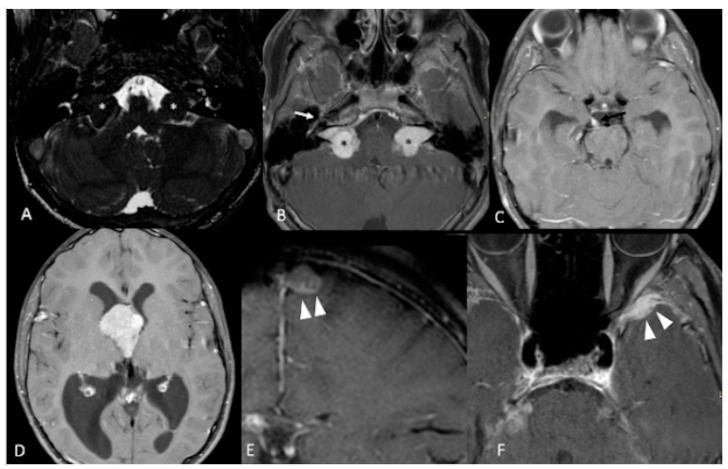
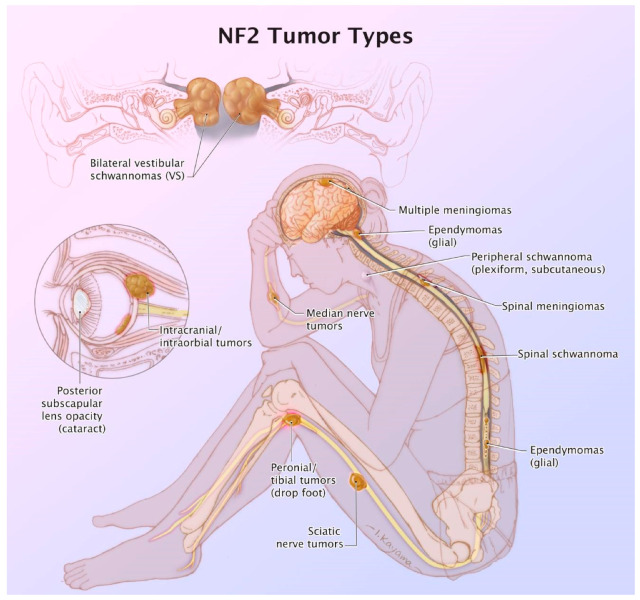
Patients diagnosed with neurofibromatosis type 2 (NF2) are extremely likely to develop meningiomas, in addition to vestibular schwannomas. Meningiomas are a common primary brain tumor; many NF2 patients suffer from multiple meningiomas. In NF2, patients have mutations in the NF2 gene, specifically with loss of function in a tumor-suppressor protein that has a number of synonymous names, including: Merlin, Neurofibromin 2, and schwannomin. Merlin is a 70 kDa protein that has 10 different isoforms. The Hippo Tumor Suppressor pathway is regulated upstream by Merlin. This pathway is critical in regulating cell proliferation and apoptosis, characteristics that are important for tumor progression. Mutations of the NF2 gene are strongly associated with NF2 diagnosis, leading to benign proliferative conditions such as vestibular schwannomas and meningiomas. Unfortunately, even though these tumors are benign, they are associated with significant morbidity and the potential for early mortality. In this review, we aim to encompass meningiomas and vestibular schwannomas as they pertain to NF2 by assessing molecular genetics, common tumor types, and tumor pathogenesis.
Keywords: meningiomas; neurofibromatosis type 2 (NF2); vestibular schwannomas.
Conflict of interest statement
Samy declares a conflict of interest due to research funding from Cochlear Corporation. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Tiwari R., Singh A.K. StatPearls. StatPearls Publishing; Treasure Island, FL, USA: 2020. Neurofibromatosis Type 2.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
