

Single-Stage Posterior Vertebral Column Resection With Circumferential Reconstruction for Thoracic/Thoracolumbar Burst Fractures With or Without Neurological Deficit: Clinical Neurological and Radiological Outcomes
- PMID: 33445964
- PMCID: PMC9344513
- DOI: 10.1177/2192568220964453
Single-Stage Posterior Vertebral Column Resection With Circumferential Reconstruction for Thoracic/Thoracolumbar Burst Fractures With or Without Neurological Deficit: Clinical Neurological and Radiological Outcomes
Abstract
Study design: Retrospective study.
Objective: The aim of this study is to evaluate the clinical, neurological, and radiological outcomes of posterior vertebral column resection (PVCR) technique for treatment of thoracic and thoracolumbar burst fractures.
Methods: Fifty-one patients (18 male, 33 female) with thoracic/thoracolumbar burst fractures who had been treated with PVCR technique were retrospectively reviewed. Preoperative and most recent radiographs were evaluated and local kyphosis angle (LKA), sagittal and coronal spinal parameters were measured. Neurological and functional results were assessed by the American Spinal Injury Association (ASIA) Impairment Scale, visual analogue scale score, Oswestry Disability Index, and Short Form 36 version 2.
Results: The mean age was 49 years (range 22-83 years). The mean follow-up period was 69 months (range 28-216 months). Fractures were thoracic in 16 and thoracolumbar in 35 of the patients. AO spine thoracolumbar injury morphological types were as follows: 1 type A3, 15 type A4, 4 type B1, 23 type B2, 8 type C injuries. PVCR was performed in a single level in 48 of the patients and in 2 levels in 3 patients. The mean operative time was 434 minutes (range 270-530 minutes) and mean intraoperative blood loss was 520 mL (range 360-1100 mL). The mean LKA improved from 34.7° to 4.9° (85.9%). For 27 patients, the initial neurological deficit (ASIA A in 8, ASIA B in 3, ASIA C in 5, and ASIA D in 11) improved at least 1 ASIA grade (1-3 grades) in 22 patients (81.5%). Solid fusion, assessed with computed tomography at the final follow-up, was achieved in all patients.
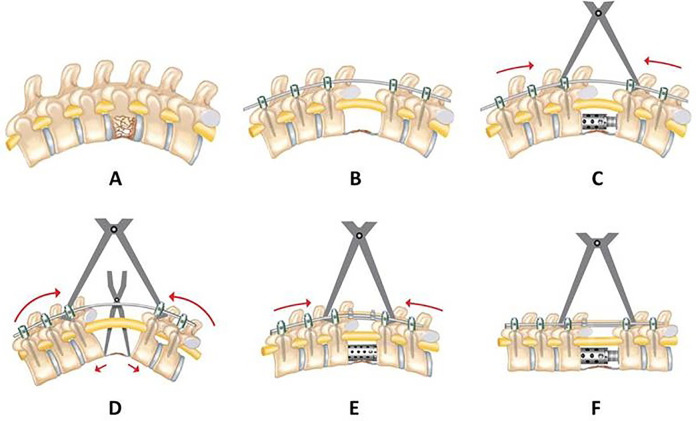
Conclusion: Single-stage PVCR provides complete spinal canal decompression, ideal kyphosis correction with gradual lengthening of anterior column together with sequential posterior column compression. Anterior column support, avoidance of the morbidity of anterior approach and improvement of neurological deficit are the other advantages of the single stage PVCR technique in patients with thoracic/thoracolumbar burst fractures.
Keywords: PVCR; burst fracture; thoracic/thoracolumbar.
Conflict of interest statement
Figures





Similar articles
-
[Posterior spinal canal decompression with screw fixation and reconstruction of three vertebral column for thoracolumbar burst fractures complicated with nerve injury].Zhongguo Gu Shang. 2018 Apr 25;31(4):322-327. doi: 10.3969/j.issn.1003-0034.2018.04.006. Zhongguo Gu Shang. 2018. PMID: 29772857 Chinese.
-
Thoracolumbar burst fractures in patients with neurological deficit: Anterior approach versus posterior percutaneous fixation with laminotomy.J Clin Neurosci. 2020 May;75:11-18. doi: 10.1016/j.jocn.2020.03.046. Epub 2020 Apr 2. J Clin Neurosci. 2020. PMID: 32249177
-
Direct reduction of thoracolumbar burst fractures by means of balloon kyphoplasty with calcium phosphate and stabilization with pedicle-screw instrumentation and fusion.Spine (Phila Pa 1976). 2008 Feb 15;33(4):E100-8. doi: 10.1097/BRS.0b013e3181646b07. Spine (Phila Pa 1976). 2008. PMID: 18277858
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Isolated unstable burst fractures of the fifth lumbar vertebra: functional and radiological outcome after posterior stabilization with reconstruction of the anterior column: About 6 cases and literature review.Orthop Traumatol Surg Res. 2020 Oct;106(6):1215-1220. doi: 10.1016/j.otsr.2020.03.014. Epub 2020 Apr 27. Orthop Traumatol Surg Res. 2020. PMID: 32354682 Review.
Cited by
-
Posterior-Only T11 Vertebral Column Resection for Pediatric Congenital Kyphosis Surgical Correction.Medicina (Kaunas). 2024 May 29;60(6):897. doi: 10.3390/medicina60060897. Medicina (Kaunas). 2024. PMID: 38929517 Free PMC article.
-
Single-Stage Posterior Unilateral Transpedicular Corpectomy With Circumferential Reconstructive Stabilization for the Treatment of Severe Thoracic and Lumbar Complete Burst Fractures.Global Spine J. 2025 Apr 25:21925682251338789. doi: 10.1177/21925682251338789. Online ahead of print. Global Spine J. 2025. PMID: 40279168 Free PMC article.
References
-
- Korovessis P, Baikousis A, Zacharatos S, Petsinis G, Koureas G, Iliopoulos P. Combined anterior plus posterior stabilization versus posterior short-segment instrumentation and fusion for mid-lumbar (L2-L4) burst fractures. Spine (Phila Pa 1976). 2006;31:859–868. - PubMed
-
- Alanay A, Acaroglu E, Yazici M, et al. Short-segment pedicle instrumentation of thoracolumbar burst fractures: does transpedicular intracorporeal grafting prevent early failure. Spine (Phila Pa 1976). 2001;26:213–217. - PubMed
-
- Alvine GF, Swain JM, Asher MA, Burton DC. Treatment of thoracolumbar burst fractures with variable screw placement or Isola instrumentation and arthrodesis: case series and literature review. J Spinal Disord Tech. 2004;17:251–264. - PubMed
-
- Vaccaro AR, Oner C, Kepler CK, et al. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine (Phila Pa 1976). 2013;38:2028–2037. - PubMed
-
- Chen HH, Wang WK, Li KC, Chen TH. Biomechanical effects of the body augmenter for reconstruction of the vertebral body. Spine (Phila Pa 1976). 2004;29:E382–E387. - PubMed
LinkOut - more resources
Full Text Sources
