

Prevalence, predictors, and mortality of bloodstream infections due to methicillin-resistant Staphylococcus aureus in patients with malignancy: systemic review and meta-analysis
- PMID: 33446122
- PMCID: PMC7809798
- DOI: 10.1186/s12879-021-05763-y
Prevalence, predictors, and mortality of bloodstream infections due to methicillin-resistant Staphylococcus aureus in patients with malignancy: systemic review and meta-analysis
Abstract
Background: Cancer patients are more likely to develop and die of bloodstream infection (BSI) than noncancer patients. Methicillin-resistant Staphylococcus aureus (MRSA), which is associated with immense mortality and economic burden worldwide, is not covered by the recommended initial antibiotic therapy for cancer patients with BSI. This systemic review was performed to estimate the global methicillin-resistant Staphylococcus aureus (MRSA) prevalence among bacteremia in patients with malignancy, and further study the predictors and mortality of cancer patients with MRSA bacteremia.
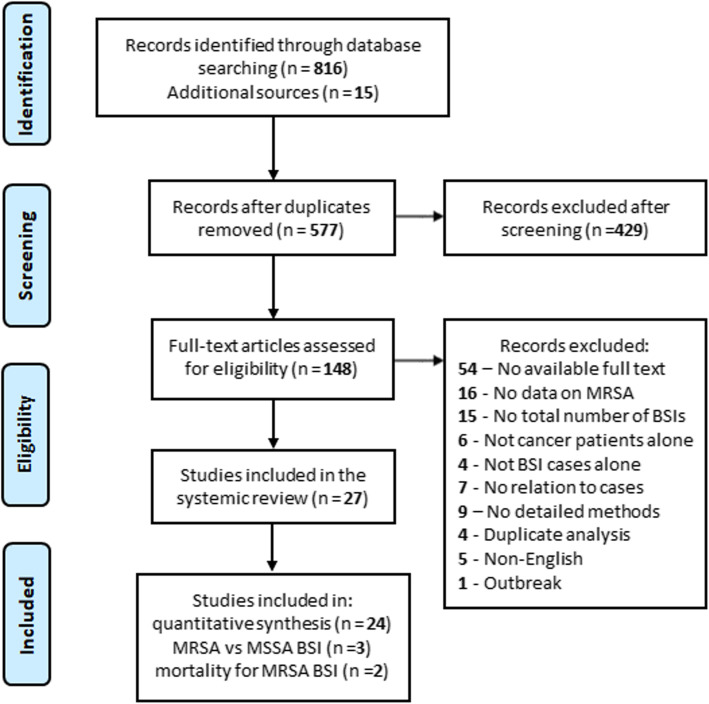
Methods: The PubMed and EMBASE databases were searched for studies published from Jan. 2000 to Mar. 2020 that provided primary data on the prevalence, predictors, or mortality of MRSA bacteremia in cancer patients. A random-effects model meta-analysis was performed to estimate the pooled prevalence of MRSA with 95% confidence intervals (95% CIs).
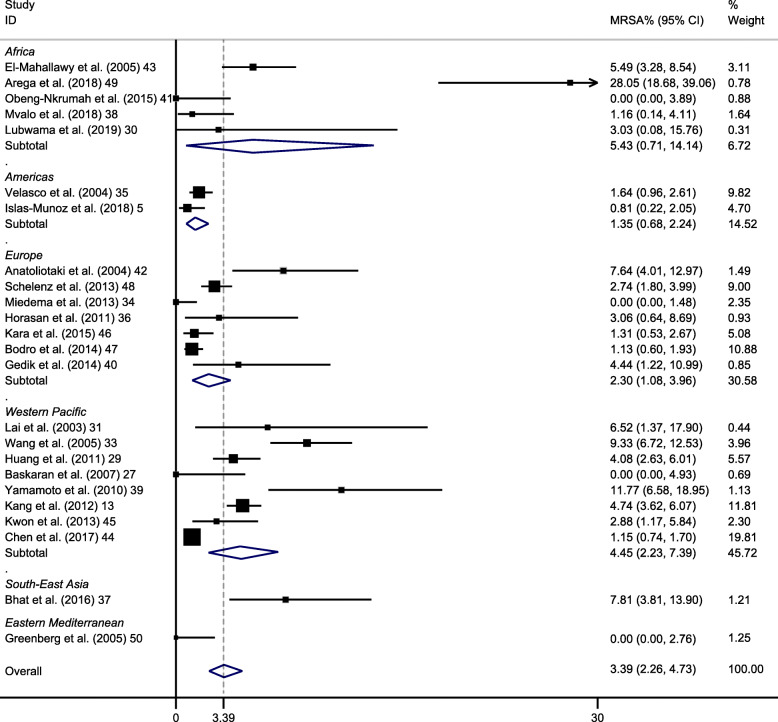
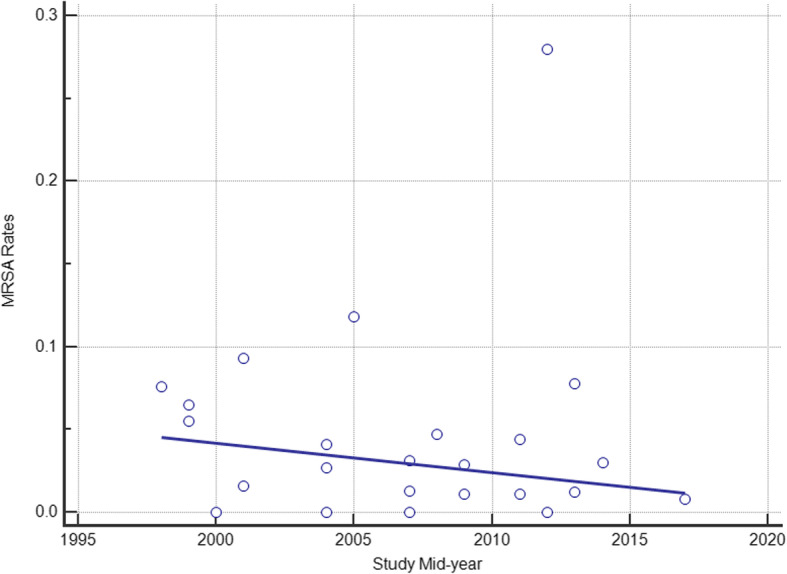
Results: The pooled prevalence of MRSA was 3% (95% CI 2-5%) among all bloodstream infections (BSIs) and 44% (95% CI 32-57%) among S. aureus bacteremia in cancer patients. Based on geographical stratification, the pooled prevalence was 5% in Africa (95% CI 1-14%), 1% in Americas (95% CI 1-2%), 2% in Europe (95% CI 1-4%), 4% in Western Pacific (95% CI 2-7%), 8% in South-east Asia (95% CI 4-14%) and 0% in Eastern Mediterranean (95% CI 0-3%). No significant temporal change in MRSA rates was detected in this analysis (R2 = 0.06; P = 0.24). Predictors for MRSA BSIs among cancer patients were identified by comparison with their methicillin-susceptible counterparts, and they were mainly related to healthcare-associated infections and immunosuppression. Finally, the 60-day mortality in adult cancer patients with MRSA BSIs was reported to be 12%, and the 6-month overall mortality was 43.2%, with community-onset infection, secondary BSI, and vancomycin MIC≥2 g/mL being the risk factors for mortality.
Conclusions: Although the prevalence of MRSA BSIs among cancer patients is relatively low, it did not decline over time as MRSA BSIs in the general hospital population and the high mortality rate was related to MRSA BSIs in patients with malignancy.
Keywords: Bacteremia; Cancer; MRSA; Methicillin-resistant Staphylococcus aureus; Prevalence.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Characteristics and outcomes of methicillin-resistant staphylococcus aureus bloodstream infections in patients with cancer treated with vancomycin: 9-year experience at a comprehensive cancer center.Oncologist. 2012;17(10):1329-36. doi: 10.1634/theoncologist.2012-0029. Epub 2012 Jun 15. Oncologist. 2012. PMID: 22707509 Free PMC article.
-
Emergence of community-associated methicillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated bloodstream infections in Korea.Infect Control Hosp Epidemiol. 2009 Feb;30(2):146-55. doi: 10.1086/593953. Infect Control Hosp Epidemiol. 2009. PMID: 19128184
-
Evolving Epidemiology of Staphylococcus aureus Bacteremia.Infect Control Hosp Epidemiol. 2015 Dec;36(12):1417-22. doi: 10.1017/ice.2015.213. Epub 2015 Sep 16. Infect Control Hosp Epidemiol. 2015. PMID: 26372679
-
Comparative effectiveness of daptomycin versus vancomycin among patients with methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections: A systematic literature review and meta-analysis.PLoS One. 2024 Feb 21;19(2):e0293423. doi: 10.1371/journal.pone.0293423. eCollection 2024. PLoS One. 2024. PMID: 38381737 Free PMC article.
-
Vancomycin or Daptomycin Plus a β-Lactam Versus Vancomycin or Daptomycin Alone for Methicillin-Resistant Staphylococcus aureus Bloodstream Infections: A Systematic Review and Meta-Analysis.Microb Drug Resist. 2021 Aug;27(8):1044-1056. doi: 10.1089/mdr.2020.0350. Epub 2021 Mar 15. Microb Drug Resist. 2021. PMID: 33728980
Cited by
-
The epidemiology of multidrug-resistant organisms in persons diagnosed with cancer in Norway, 2008-2018: expanding surveillance using existing laboratory and register data.Eur J Clin Microbiol Infect Dis. 2024 Jan;43(1):121-132. doi: 10.1007/s10096-023-04698-3. Epub 2023 Nov 18. Eur J Clin Microbiol Infect Dis. 2024. PMID: 37980302 Free PMC article.
-
Transcriptional Landscapes of Herelleviridae Bacteriophages and Staphylococcus aureus during Phage Infection: An Overview.Viruses. 2023 Jun 23;15(7):1427. doi: 10.3390/v15071427. Viruses. 2023. PMID: 37515114 Free PMC article. Review.
-
Glucomannan enhanced the macrophage activity in exposure to methicillin-resistant Staphylococcus aureus (MRSA): in-vitro study.Iran J Microbiol. 2023 Aug;15(4):557-564. doi: 10.18502/ijm.v15i4.13510. Iran J Microbiol. 2023. PMID: 38045713 Free PMC article.
-
Clinical characteristics of and risk factors for secondary bloodstream infection after pneumonia among patients infected with methicillin-resistant Staphylococcus aureus.Heliyon. 2022 Dec 2;8(12):e11978. doi: 10.1016/j.heliyon.2022.e11978. eCollection 2022 Dec. Heliyon. 2022. PMID: 36506352 Free PMC article.
-
Pandemic clone USA300 in a Brazilian hospital: detection of an emergent lineage among methicillin-resistant Staphylococcus aureus isolates from bloodstream infections.Antimicrob Resist Infect Control. 2022 Sep 14;11(1):114. doi: 10.1186/s13756-022-01154-3. Antimicrob Resist Infect Control. 2022. PMID: 36104710 Free PMC article.
References
-
- Hsieh RW, Schrank GM, Hsu WT, Su KY, Lee CC. Temporal trend of microbiological profiles among patients with bloodstream infections: A comparison between cancer and noncancer patients in a nationwide database. J Clin Oncol. 2019;37.
-
- Macedo F, Monteiro AR, Soares R, Pereira T, Bonito N, Sousa G. Bacteremia in oncologic patients and multi drug resistant microorganisms: A growing issue. Support Care Cancer. 2019;27(1):S139. doi: 10.1007/s00520-018-4298-7. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
