

Short-term effectiveness of precise safety decompression via double percutaneous lumbar foraminoplasty and percutaneous endoscopic lumbar decompression for lateral lumbar spinal canal stenosis: a prospective cohort study
- PMID: 33446166
- PMCID: PMC7807700
- DOI: 10.1186/s12891-021-03956-9
Short-term effectiveness of precise safety decompression via double percutaneous lumbar foraminoplasty and percutaneous endoscopic lumbar decompression for lateral lumbar spinal canal stenosis: a prospective cohort study
Abstract
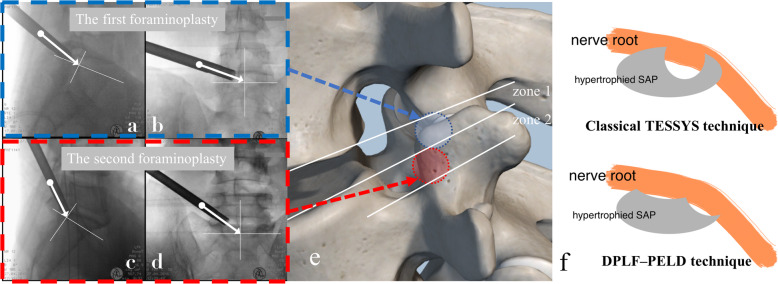
Purpose: This prospective cohort study reports on a modified technique, namely precise safety decompression via double percutaneous lumbar foraminoplasty (DPLF) and percutaneous endoscopic lumbar decompression (PELD) for lateral lumbar spinal canal (LLSC) stenosis, and its short-term clinical outcomes.
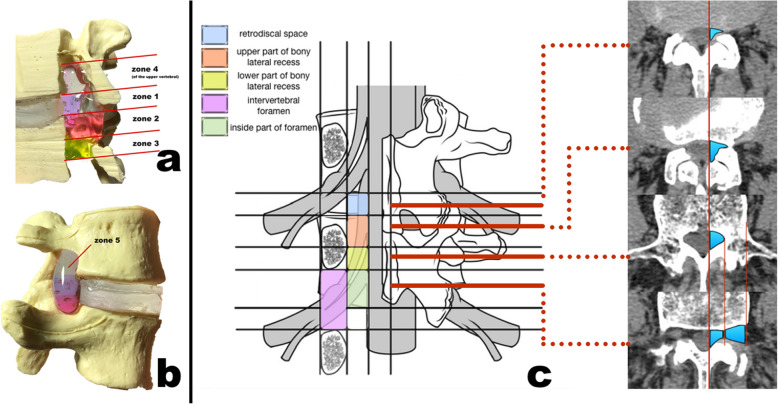
Methods: The study analyzed 69 patients with single-level LLSC stenosis simultaneously occurring in both zones 1 and 2 (defined as retrodiscal space and upper bony lateral recess respectively by new LLSC classification) who underwent DPLF-PELD from November 2018 to April 2019. Clinical outcomes were evaluated according to preoperative, 3 months postoperatively, and last follow-up, via leg pain/low back pain (LBP) visual analog scale (VAS) scores, Oswestry disability index (ODI) scores, and the Macnab criteria. The postoperative MRI and CT were used to confirm the complete decompression, and flexion-extension x-rays at the last follow-up were used to observe lumbar stability.
Results: All patients successfully underwent DPLF-PELD, and the stenosis was completely decompressed, confirmed by postoperative MRI and CT. The mean follow-up duration was 13 months (range: 8-17 months). The mean preoperative leg pain VAS score is 7.05 ± 1.04 (range 5-9), which decreased to 1.03 ± 0.79(range: 0-3) at 3 months postoperatively and to 0.75 ± 0.63 (range: 0-2) by the last follow-up visit (p < 0.05). The mean preoperative ODI was 69.8 ± 9.05 (range: 52-85), which decreased to 20.3 ± 5.52 (range: 10-35) at the third month postoperatively and to 19.6 ± 5.21 (range: 10-34) by the final follow-up visit (p < 0.05). The satisfactory (excellent or good) results were 94.2%. There was one patient with aggravated symptoms, which were relieved after an open surgery. Two patients had a dural tear, and two patients suffered postoperative LBP. No recurrence or segmental instability was observed at the final follow-up.
Conclusion: DPLF-PELD could be a good alternative for the treatment of LLSC stenosis patients whose stenosis occurred in both zones 1 and 2.
Trial registration: Chinese Clinical Trial Registry ( ChiCTR1800019551 ). Registered 18 November 2018.
Keywords: Double percutaneous lumbar foraminoplasty; Lumbar lateral spinal canal; Percutaneous endoscopic lumbar decompression.
Conflict of interest statement
All authors declare no conflict of interest.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
