

Efficacy of plasma exchange for antineutrophil cytoplasmic antibody-associated systemic vasculitis: a systematic review and meta-analysis
- PMID: 33446268
- PMCID: PMC7809754
- DOI: 10.1186/s13075-021-02415-z
Efficacy of plasma exchange for antineutrophil cytoplasmic antibody-associated systemic vasculitis: a systematic review and meta-analysis
Abstract
Objective: To assess through systematic review and meta-analysis whether plasma exchange (PE) is associated with prognosis in antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) patients.
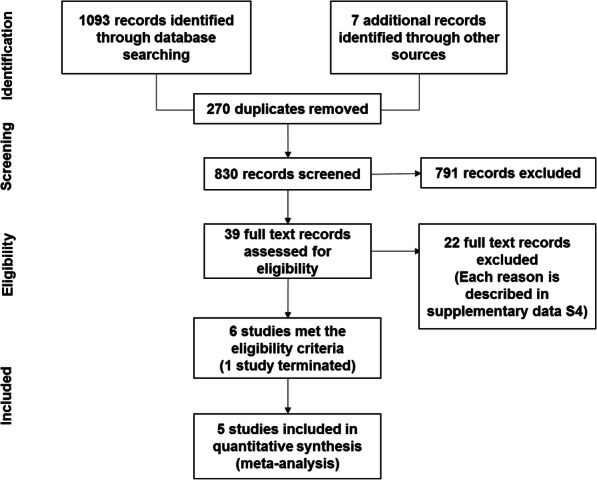
Methods: A systematic search of PubMed, MEDLINE, Embase, and CENTRAL databases from inception to 17 June 2020 was conducted. Ongoing or unpublished trials were also searched in ClinicalTrials.gov and the World Health Organization trials portal. Randomised controlled trials (RCTs) comparing PE vs. non-PE in AAV patients (microscopic polyangiitis [MPA], granulomatosis with polyangiitis [GPA], or eosinophilic granulomatosis with polyangiitis [EGPA]) were included. The combined risk ratio (RR) was calculated by the random-effects model using the Mantel-Haenszel method. Heterogeneity was measured using the I2 statistic. Primary outcomes were mortality, clinical remission (CR), and adverse events (AEs).
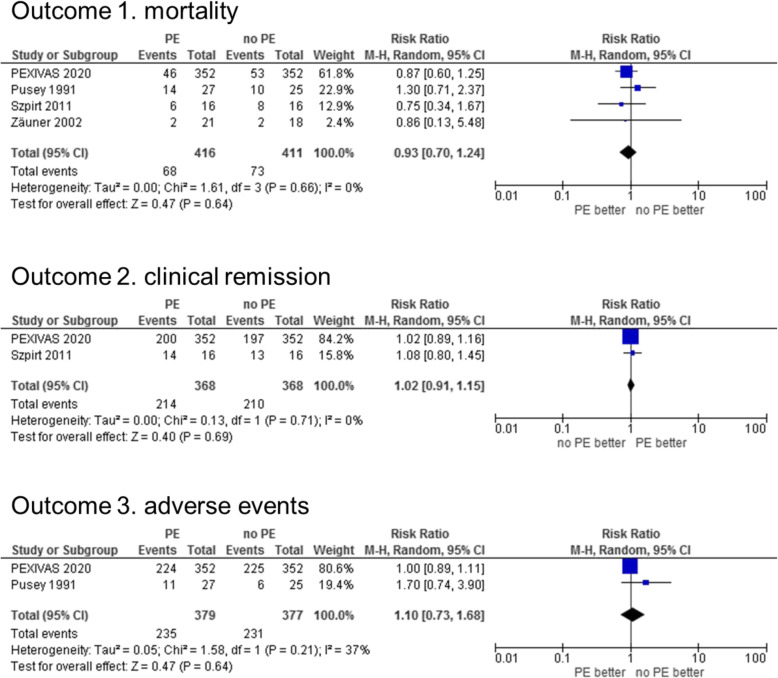
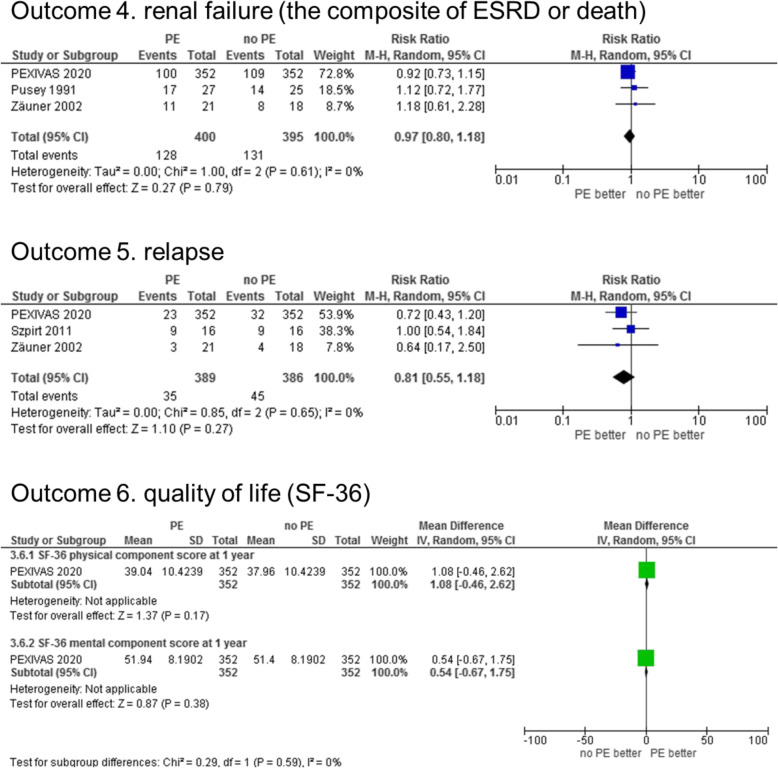
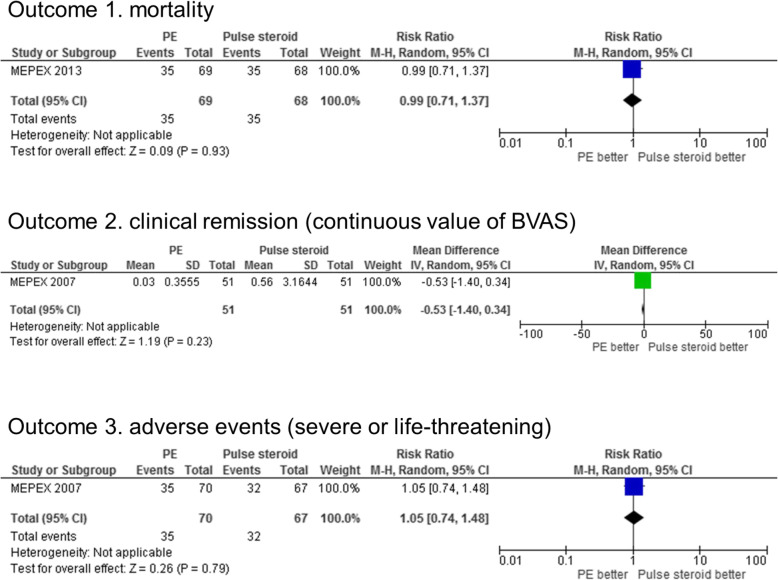
Results: Four RCTs comparing PE vs. no PE (N = 827) and 1 RCT comparing PE vs. pulse steroid treatment (N = 137) were included. All participants were MPA or GPA patients (no EGPA patients). PE was not associated with main primary outcomes compared with no PE (mortality RR 0.93 [95% confidence interval {CI} 0.70-1.24], I2 = 0%; CR RR 1.02 [95% CI 0.91-1.15], I2 = 0%; and AE RR 1.10 [95% CI 0.73-1.68], I2 = 37%) or pulse steroid (mortality RR 0.99 [95% CI 0.71-1.37]; CR [the Birmingham Vasculitis Activity score] mean difference - 0.53 [95% CI - 1.40-0.34]; and AE RR 1.05 [95% CI 0.74-1.48]). Focusing on the early treatment phases, PE was associated with a reduction in end-stage renal disease incidence compared with both no PE (PE 1/43 vs. no PE 10/41; RR 0.14 [0.03-0.77] at 3 months) and pulse steroid (PE 11/70 vs. pulse steroid 23/67; RR 0.46 [0.24-0.86] at 3 months).
Conclusion: We carried out a systematic review and meta-analysis targeting all AAV patients, including MPA, GPA, and EGPA. In AAV patients, performing PE was not associated with the risk of mortality, CR, and AE. No RCT exists evaluating the efficacy of PE for EGPA; hence, this is required in the future. The results may affect the development of guidelines for AAV and may indicate the direction of future clinical research on AAV.
Trial registration: UMIN R000045239 , PROSPERO CRD42020182566 .
Keywords: Churg-Strauss syndrome; Granulomatosis with polyangiitis; Meta-analysis; Microscopic polyangiitis; Plasma exchange.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The role of tobacco smoking in anti-neutrophil cytoplasmic antibody-associated vasculitis: a systematic review.Clin Exp Rheumatol. 2024 Jul;42(7):1321-1332. doi: 10.55563/clinexprheumatol/nu8ngr. Epub 2024 Jul 4. Clin Exp Rheumatol. 2024. PMID: 38976289
-
Electronic cigarettes for smoking cessation.Cochrane Database Syst Rev. 2021 Sep 14;9(9):CD010216. doi: 10.1002/14651858.CD010216.pub6. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 Nov 17;11:CD010216. doi: 10.1002/14651858.CD010216.pub7. PMID: 34519354 Free PMC article. Updated.
-
Electronic cigarettes for smoking cessation.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD010216. doi: 10.1002/14651858.CD010216.pub7. Cochrane Database Syst Rev. 2022. Update in: Cochrane Database Syst Rev. 2024 Jan 8;1:CD010216. doi: 10.1002/14651858.CD010216.pub8. PMID: 36384212 Free PMC article. Updated.
-
Performance of MPO-ANCA and PR3-ANCA immunoassays for the stratification of specific ANCA-associated vasculitis: A systematic review and meta-analysis.Autoimmun Rev. 2022 Jun;21(6):103100. doi: 10.1016/j.autrev.2022.103100. Epub 2022 Apr 19. Autoimmun Rev. 2022. PMID: 35452854
-
SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19.Cochrane Database Syst Rev. 2021 Sep 2;9(9):CD013825. doi: 10.1002/14651858.CD013825.pub2. Cochrane Database Syst Rev. 2021. PMID: 34473343 Free PMC article.
Cited by
-
Is There Still a Role of Plasma Exchange in the Current Management of ANCA-Associated Vasculitides?Curr Rheumatol Rep. 2022 Apr;24(4):111-117. doi: 10.1007/s11926-022-01064-8. Epub 2022 Mar 22. Curr Rheumatol Rep. 2022. PMID: 35316496 Free PMC article. Review.
-
Time-dependent risk of mortality and end-stage kidney disease among patients with granulomatosis with polyangiitis.Front Med (Lausanne). 2022 Aug 10;9:817204. doi: 10.3389/fmed.2022.817204. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36035421 Free PMC article.
-
Evidence-Based Guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis.Nat Rev Rheumatol. 2023 Jun;19(6):378-393. doi: 10.1038/s41584-023-00958-w. Epub 2023 May 9. Nat Rev Rheumatol. 2023. PMID: 37161084 Review.
-
Management of antineutrophil cytoplasmic antibody-associated vasculitis with glomerulonephritis as proposed by the ACR 2021, EULAR 2022 and KDIGO 2021 guidelines/recommendations.Nephrol Dial Transplant. 2023 Oct 31;38(11):2637-2651. doi: 10.1093/ndt/gfad090. Nephrol Dial Transplant. 2023. PMID: 37164940 Free PMC article.
-
Efficacy of protein A immunoadsorption and therapeutic plasma exchange in ANCA-associated vasculitis with severe renal involvement: a retrospective study.Ann Med. 2023 Dec;55(1):2230875. doi: 10.1080/07853890.2023.2230875. Ann Med. 2023. PMID: 37452682 Free PMC article.
References
-
- Harigai M, Nagasaka K, Amano K, Bando M, Dobashi H, Kawakami T, et al. 2017 Clinical practice guidelines of the Japan Research Committee of the Ministry of Health, Labour, and Welfare for Intractable Vasculitis for the management of ANCA-associated vasculitis. Mod Rheumatol. 2019;29(1):20–30. doi: 10.1080/14397595.2018.1500437. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
