

CT image segmentation for inflamed and fibrotic lungs using a multi-resolution convolutional neural network
- PMID: 33446781
- PMCID: PMC7809065
- DOI: 10.1038/s41598-020-80936-4
CT image segmentation for inflamed and fibrotic lungs using a multi-resolution convolutional neural network
Abstract
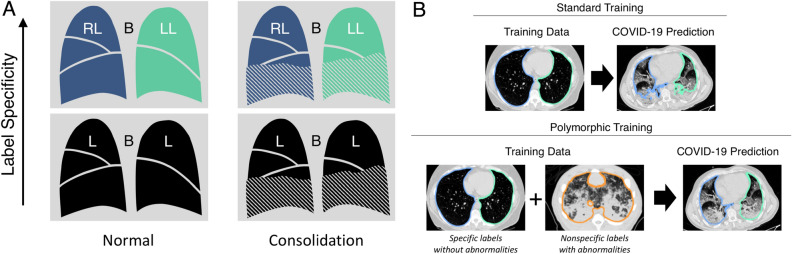
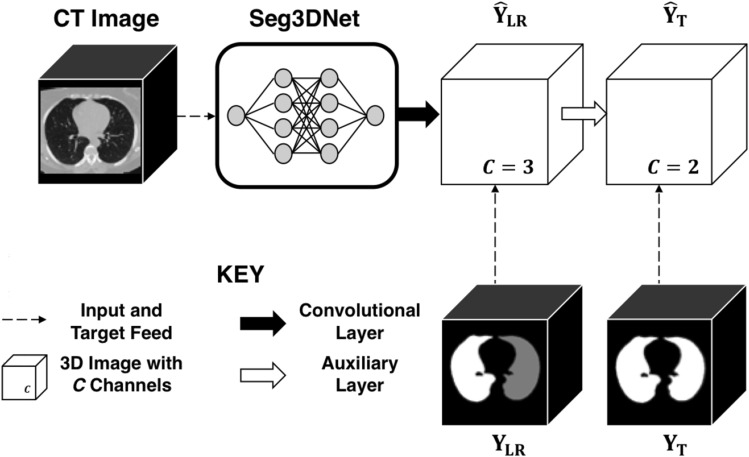
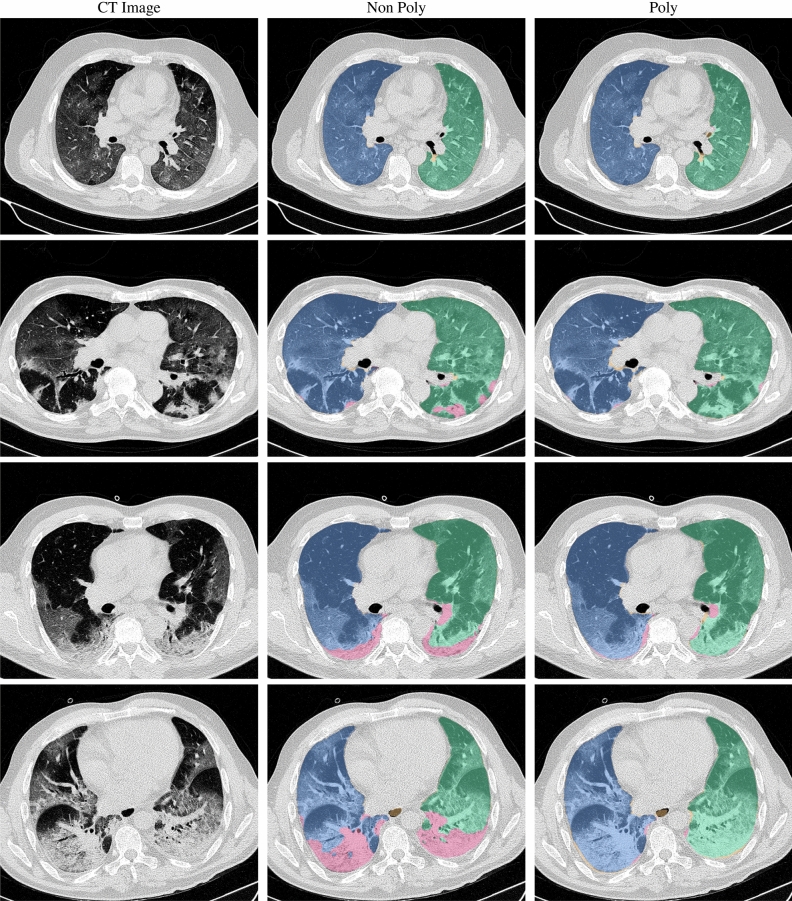
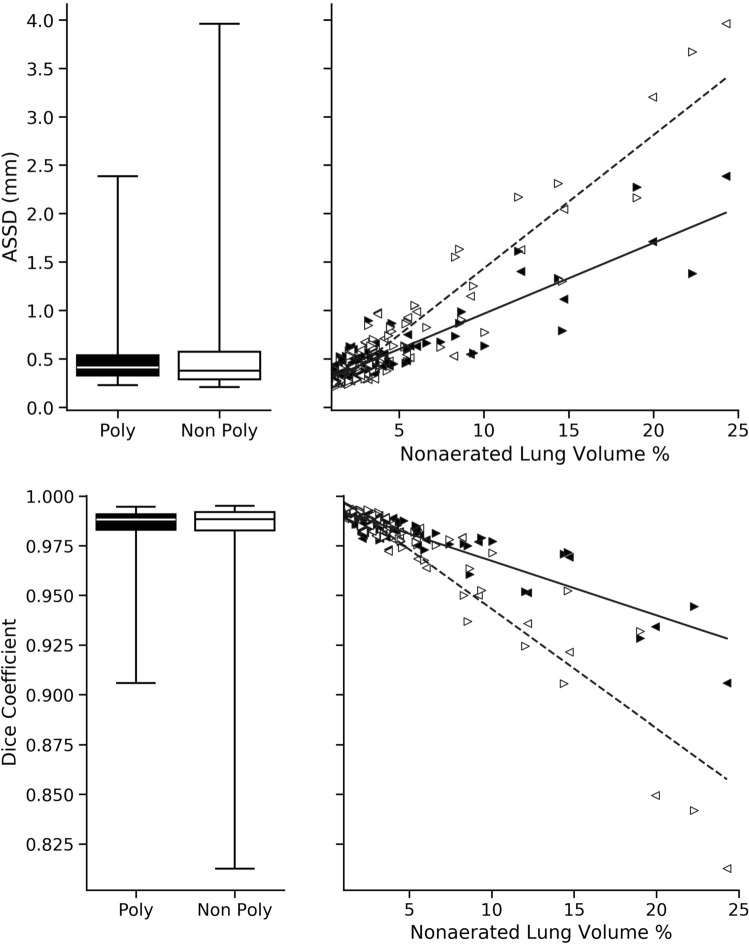
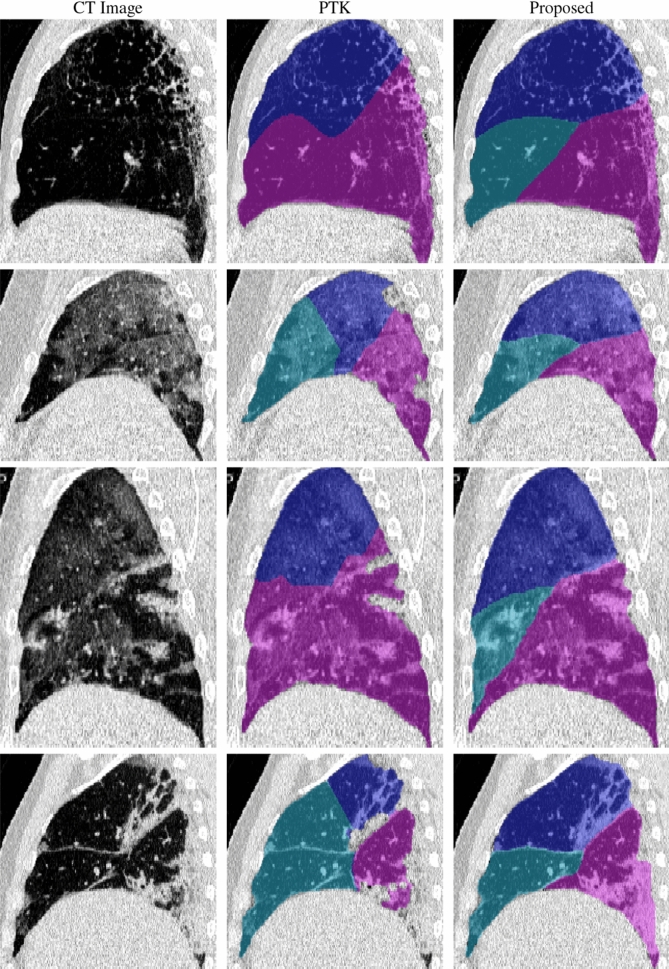
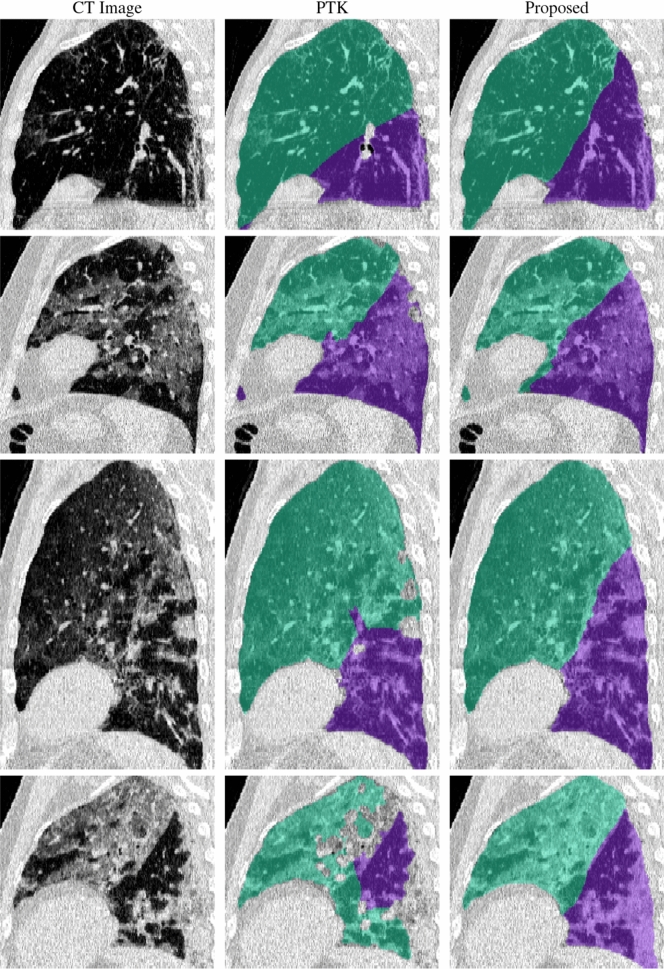
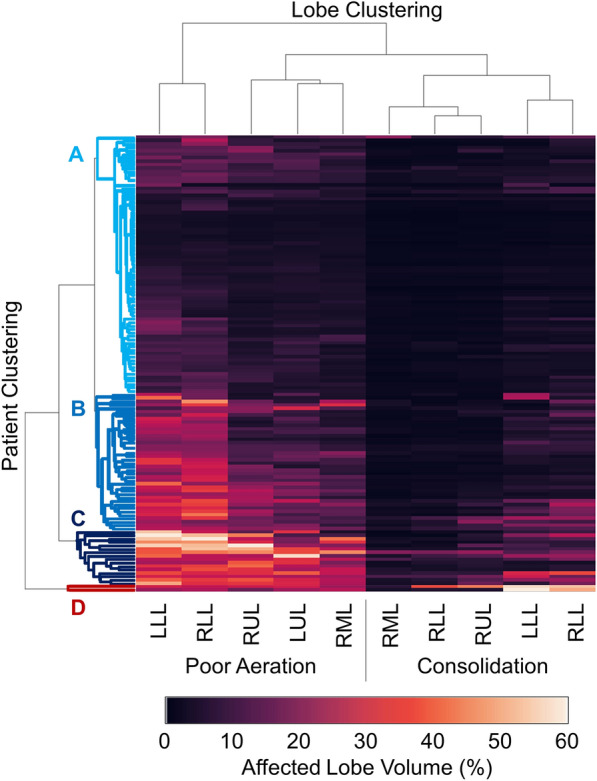
The purpose of this study was to develop a fully-automated segmentation algorithm, robust to various density enhancing lung abnormalities, to facilitate rapid quantitative analysis of computed tomography images. A polymorphic training approach is proposed, in which both specifically labeled left and right lungs of humans with COPD, and nonspecifically labeled lungs of animals with acute lung injury, were incorporated into training a single neural network. The resulting network is intended for predicting left and right lung regions in humans with or without diffuse opacification and consolidation. Performance of the proposed lung segmentation algorithm was extensively evaluated on CT scans of subjects with COPD, confirmed COVID-19, lung cancer, and IPF, despite no labeled training data of the latter three diseases. Lobar segmentations were obtained using the left and right lung segmentation as input to the LobeNet algorithm. Regional lobar analysis was performed using hierarchical clustering to identify radiographic subtypes of COVID-19. The proposed lung segmentation algorithm was quantitatively evaluated using semi-automated and manually-corrected segmentations in 87 COVID-19 CT images, achieving an average symmetric surface distance of [Formula: see text] mm and Dice coefficient of [Formula: see text]. Hierarchical clustering identified four radiographical phenotypes of COVID-19 based on lobar fractions of consolidated and poorly aerated tissue. Lower left and lower right lobes were consistently more afflicted with poor aeration and consolidation. However, the most severe cases demonstrated involvement of all lobes. The polymorphic training approach was able to accurately segment COVID-19 cases with diffuse consolidation without requiring COVID-19 cases for training.
Conflict of interest statement
Drs. Hoffman and Reinhardt are co-founders and shareholders in VIDA Diagnostics, Inc., a medical imaging software spin-off from the University of Iowa. Dr. Guo is a shareholder in VIDA Diagnostics, Inc. Drs. Kaczka and Herrmann are co-founders and shareholders of OscillaVent, Inc. Dr. Gerard has no competing interests. Yi Xin has no competing interests. Kevin T. Martin has no competing interests. Dr. Rezoagli has no competing interests. Dr. Ippolito has no competing interests. Dr. Bellani has no competing interests. Dr. Cereda has no competing interests.
Figures
Update of
-
CT Image Segmentation for Inflamed and Fibrotic Lungs Using a Multi-Resolution Convolutional Neural Network.ArXiv [Preprint]. 2021 Jan 14:arXiv:2010.08582v2. ArXiv. 2021. Update in: Sci Rep. 2021 Jan 14;11(1):1455. doi: 10.1038/s41598-020-80936-4. PMID: 33469558 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
