

Role of prenatal imaging in the diagnosis and management of fetal facio-cervical masses
- PMID: 33446872
- PMCID: PMC7809128
- DOI: 10.1038/s41598-021-80976-4
Role of prenatal imaging in the diagnosis and management of fetal facio-cervical masses
Abstract
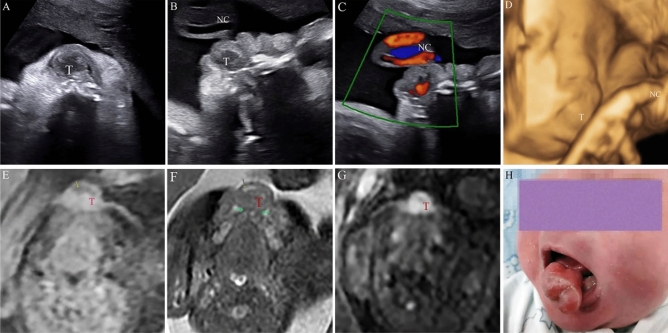
Congenital facio-cervical masses can be a developmental anomaly of cystic, solid, or vascular origin, and have an inseparable relationship with adverse prognosis. This retrospective cross-sectional study aimed at determining on the prenatal diagnosis of congenital facio-cervical masses, its management and outcome in a large tertiary referral center. We collected information on prenatal clinical data, pregnancy outcomes, survival information, and final diagnosis. Out of 130 cases of facio-cervical masses, a total of 119 cases of lymphatic malformations (LMs), 2 cases of teratoma, 2 cases of thyroglossal duct cyst, 4 cases of hemangioma, 1 case of congenital epulis, and 2 cases of dermoid cyst were reviewed. The accuracy of prenatal ultrasound was 93.85% (122/130). Observations of diameters using prenatal ultrasound revealed that the bigger the initial diameter is, the bigger the relative change during pregnancy. Magnetic resonance imaging (MRI) revealed that 2 cases of masses were associated with airway compression. In conclusion, ultrasound has a high overall diagnostic accuracy of fetal face and neck deformities. Prenatal US can enhance the management of ambulatory monitoring and classification. Furthermore, MRI provided a detailed assessment of fetal congenital malformations, as well as visualization of the trachea, presenting a multi-dimensional anatomical relationship.
Conflict of interest statement
The authors declare no competing interests.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
