

Effect of Modified Uvulopalatopharyngoplasty without Tonsillectomy on Obstructive Sleep Apnea: Polysomnographic Outcome and Correlation with Drug-Induced Sleep Endoscopy
- PMID: 33447114
- PMCID: PMC7802905
- DOI: 10.2147/NSS.S286203
Effect of Modified Uvulopalatopharyngoplasty without Tonsillectomy on Obstructive Sleep Apnea: Polysomnographic Outcome and Correlation with Drug-Induced Sleep Endoscopy
Abstract
Objective: Uvulopalatopharyngoplasty (UPPP) is a common procedure for the treatment of obstructive sleep apnea (OSA) and is usually initiated with the resection of palatine tonsils. Because tonsillectomy potentially contributes to complications, minimally invasive upper airway surgeries have been proposed for OSA therapy. Whether tonsillectomy is always essential for UPPP remains unclear, particularly for patients with small tonsils. The purpose of this study was to present the effect of modified UPPP without tonsillectomy (UPsT) on patients with OSA and attempt to select the candidates for this procedure.
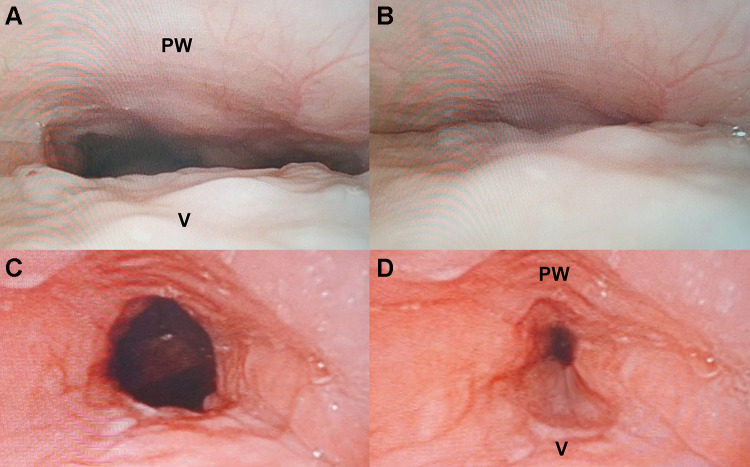
Methods: This is a retrospective cohort study of patients with OSA, with tonsil size of grade 0-2, and with only retropalatal obstruction in drug-induced sleep endoscopy (DISE). The patients underwent UPsT at a tertiary center from November 2017 to December 2019. The sleep study was performed before and at least 3 months after surgery. The demographics, surgical outcomes, and staging patterns of preoperative DISE were recorded. The correlation between surgical outcome and DISE was also established.
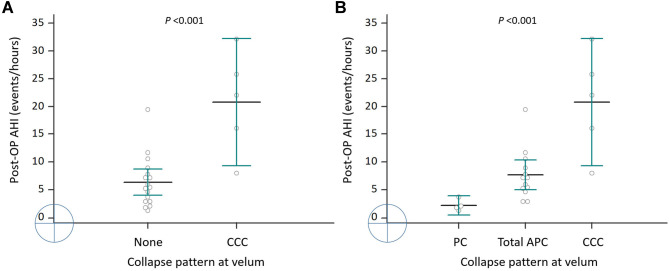
Results: A total of 22 adults with an average age of 46.5 years [interquartile range: 40 to 60 years] completed the follow-up study. Their apnea-hypopnea index (AHI) and Epworth sleepiness scale values improved significantly after surgery. Of the 17 patients with partial collapse and complete anteroposterior collapse (APC) at the velum, 16 presented good responses to UPsT. However, among the five patients with complete concentric collapse (CCC), only two (2/5, 40%) satisfied the criteria for surgical success. Furthermore, their follow-up AHI values were significantly higher than those of patients without CCC in DISE.
Conclusion: UPsT was demonstrated to be an effective therapy for patients with OSA who had small tonsils and retropalatal obstruction in DISE. CCC in sleep endoscopy indicates a poorer surgical outcome than does complete APC and partial collapse at the velum.
Keywords: complete concentric collapse; drug-induced sleep endoscopy; lateral pharyngoplasty; obstructive sleep apnea; suspension palatoplasty; tonsillectomy; uvulopalatopharyngoplasty.
© 2021 Chiu et al.
Conflict of interest statement
The authors declare no conflicts of interest for this work.
Figures

Similar articles
-
The role of drug-induced sleep endoscopy: predicting and guiding upper airway surgery for adult OSA patients.Sleep Breath. 2018 Dec;22(4):925-931. doi: 10.1007/s11325-018-1730-7. Epub 2018 Oct 1. Sleep Breath. 2018. PMID: 30276710
-
Post-Operative Sleep Endoscopy with Target-Controlled Infusion After Palatopharyngoplasty for Obstructive Sleep Apnea: Anatomical and Polysomnographic Outcomes.Nat Sci Sleep. 2021 Jul 20;13:1181-1193. doi: 10.2147/NSS.S311702. eCollection 2021. Nat Sci Sleep. 2021. PMID: 34321943 Free PMC article.
-
Combined Transoral Robotic Tongue Base Surgery and Palate Surgery in Obstructive Sleep Apnea Syndrome: Modified Uvulopalatopharyngoplasty versus Barbed Reposition Pharyngoplasty.J Clin Med. 2021 Jul 18;10(14):3169. doi: 10.3390/jcm10143169. J Clin Med. 2021. PMID: 34300335 Free PMC article.
-
Surgical failure guided by DISE in patients with obstructive sleep apnea: a systematic review and meta-analysis.Eur Arch Otorhinolaryngol. 2024 Jul;281(7):3333-3343. doi: 10.1007/s00405-024-08484-5. Epub 2024 Feb 7. Eur Arch Otorhinolaryngol. 2024. PMID: 38324055
-
Drug induced sleep endoscopy in the decision-making process of children with obstructive sleep apnea.Sleep Med. 2015 Mar;16(3):331-5. doi: 10.1016/j.sleep.2014.10.017. Epub 2015 Jan 20. Sleep Med. 2015. PMID: 25754384 Review.
Cited by
-
Is there a relationship between tonsil volume and the success of pharyngeal surgery among adult patients with obstructive sleep apnea?Braz J Otorhinolaryngol. 2022 Nov-Dec;88 Suppl 5(Suppl 5):S156-S161. doi: 10.1016/j.bjorl.2021.12.002. Epub 2022 Jan 4. Braz J Otorhinolaryngol. 2022. PMID: 35184978 Free PMC article.
-
TORS as Part of Multilevel Surgery in OSA: The Importance of Careful Patient Selection and Outcomes.J Clin Med. 2022 Feb 14;11(4):990. doi: 10.3390/jcm11040990. J Clin Med. 2022. PMID: 35207264 Free PMC article.
-
New non-invasive electrical stimulation devices for treatment of snoring and obstructive sleep apnoea: a systematic review.Sleep Breath. 2023 Mar;27(1):103-108. doi: 10.1007/s11325-022-02615-0. Epub 2022 Apr 23. Sleep Breath. 2023. PMID: 35460429
-
No-cutting remodelling intra-pharyngeal surgery can avoid CPAP in selected OSA patients: myth or reality?Eur Arch Otorhinolaryngol. 2022 Oct;279(10):5039-5045. doi: 10.1007/s00405-022-07261-6. Epub 2022 Feb 6. Eur Arch Otorhinolaryngol. 2022. PMID: 35124744
-
A New Lighting System for Surgical Vision Optimization in Barbed Pharyngoplasty for OSA.J Pers Med. 2023 Aug 28;13(9):1320. doi: 10.3390/jpm13091320. J Pers Med. 2023. PMID: 37763089 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
