

What Are the Predictors of Poor Patient-Reported Outcomes After Shoulder Instability Surgery?
- PMID: 33447618
- PMCID: PMC7780330
- DOI: 10.1177/2325967120966343
What Are the Predictors of Poor Patient-Reported Outcomes After Shoulder Instability Surgery?
Abstract
Background: Prospectively collected responses to Patient Acceptable Symptom State (PASS) questions after shoulder instability surgery are limited. Responses to these outcome measures are imperative to understanding their clinical utility.
Purpose/hypothesis: The purpose of this study was to evaluate which factors predict unfavorable patient-reported outcomes after shoulder instability surgery, including "no" to the PASS question. We hypothesized that poor outcomes would be associated with male adolescents, bone loss, combined labral tears, and articular cartilage injuries.
Study design: Cohort study; Level of evidence, 2.
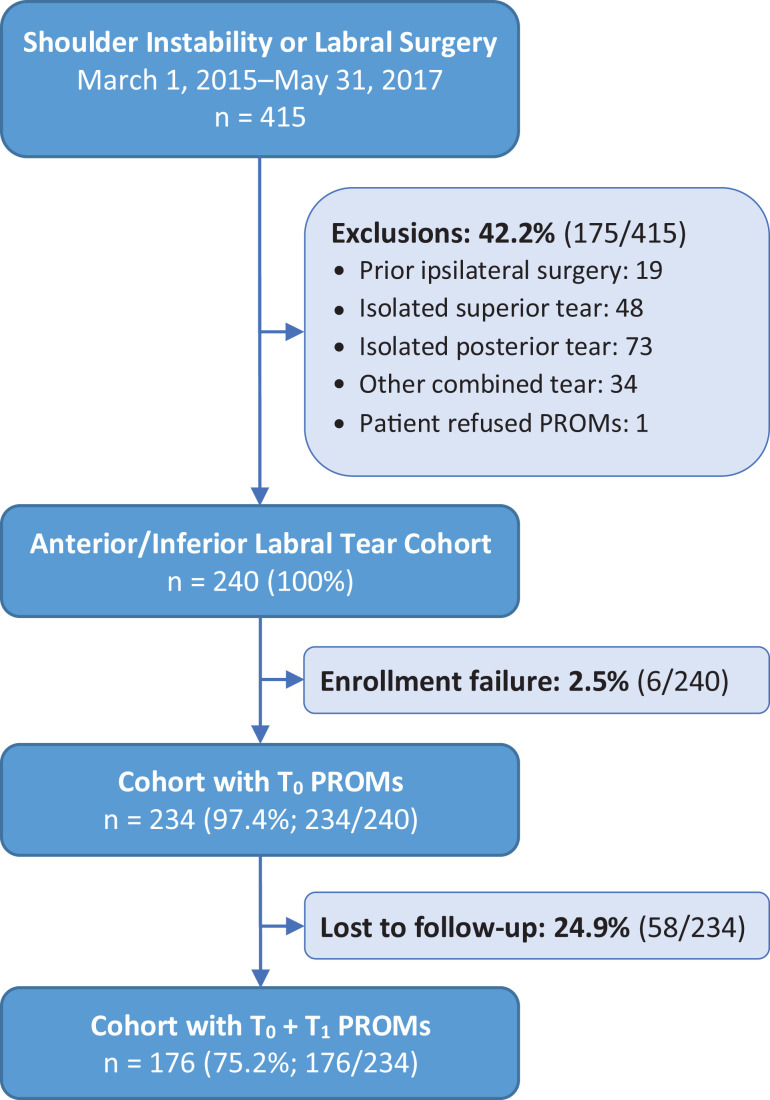
Methods: Patients aged ≥13 years undergoing shoulder instability surgery were included in point-of-care data collection at a single institution across 12 surgeons between 2015 and 2017. Patients with anterior-inferior labral tears were included, and those with previous ipsilateral shoulder surgery were excluded. Demographics, American Shoulder and Elbow Surgeons (ASES) and Single Assessment Numeric Evaluation (SANE) scores, and surgical findings were obtained at baseline. ASES and SANE scores, PASS responses, and early revision surgery rates were obtained at a minimum of 1 year after the surgical intervention. Regression analyses were performed.
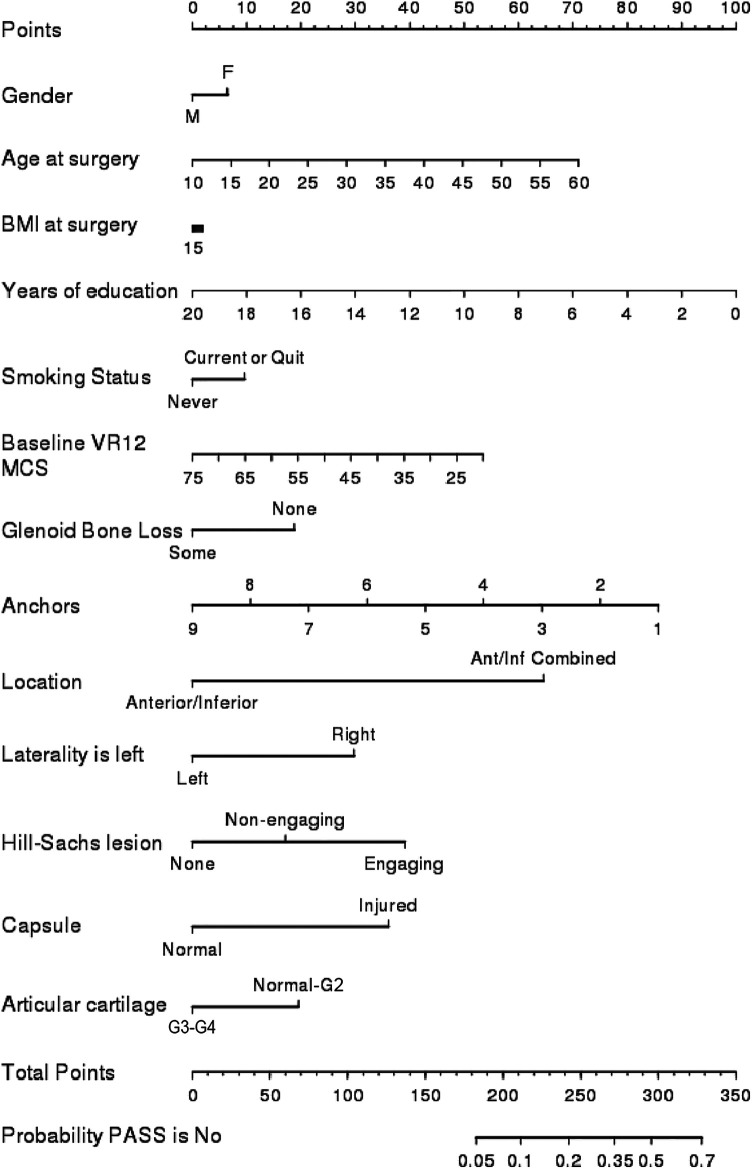
Results: A total of 234 patients met inclusion criteria, of which 176 completed follow-up responses (75.2%). Nonresponders had a younger age, greater frequency of glenoid bone loss, fewer combined tears, and more articular cartilage injuries (P < .05). Responders' mean age was 25.1 years, and 22.2% were female. Early revision surgery occurred in 3.4% of these patients, and 76.1% responded yes to the PASS question. A yes response correlated with a mean 25-point improvement in the ASES score and a 40-point improvement in the SANE score. On multivariate analysis, combined labral tears (anterior-inferior plus superior or posterior tears) were associated with greater odds of responding no to the PASS question, while both combined tears and injured capsules were associated with lower ASES and SANE scores (P < .05). Sex, bone loss, and grade 3 to 4 articular cartilage injuries were not associated with variations on any patient-reported outcome measure.
Conclusion: Patients largely approved of their symptom state at ≥1 year after shoulder instability surgery. A response of yes to the PASS question was given by 76.1% of patients and was correlated with clinically and statistically significant improvements in ASES and SANE scores. Combined labral tears and injured capsules were negative prognosticators across patient-reported outcome measures, whereas sex, bone loss, and cartilage injuries were not.
Keywords: PROMs; follow-up; instability; patient-reported outcome measures; shoulder.
© The Author(s) 2020.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Research reported in this publication was partially supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under award number K23AR066133, which supported a portion of M.H.J.’s professional effort. A.F.B. has received educational support from Smith & Nephew. M.S.S. has received consulting fees and nonconsulting fees from Arthrex. L.D.F. has received consulting fees from Zimmer Biomet and hospitality payments from the Musculoskeletal Transplant Foundation. M.H.J. is on the scientific advisory board for Samumed. B.W.M. has received educational support from Arthrex and hospitality payments from Rock Medical and Zimmer Biomet. A.M. has received educational support from Rock Medical; consulting fees from Amniox Medical, Arthrosurface, Linvatec, Stryker, and Trice; speaking fees from Trice; royalties from Arthrosurface, Wolters Kluwer, and Zimmer Biomet; honoraria from Arthrosurface; and hospitality payments from Arthrex, DJO, and Smith & Nephew and has stock in Arthrosurface and Trice. E.T.R. has received research support from DePuy; consulting fees from DJO, DePuy, and Encore Medical; royalties from DJO; and honoraria from DePuy and DJO. J.T.R. has received educational consulting fees from Smith & Nephew. K.P.S. has received research support from DJO and Smith & Nephew and consulting fees from Cytori Therapeutics, Flexion Therapeutics, Mitek, the National Football League, and Samumed. K.L.S. has received educational support from Arthrex and Biomet; consulting fees from Molnlycke Health Care; honoraria from Fidia Pharma; and hospitality payments from Horizon Pharma, the Musculoskeletal Transplant Foundation, Ramsay Medical, and Stryker. J.W. has received educational support from Arthrex. P.M.S. has received educational support from Rock Medical; consulting fees from Arthrex, DJO, and DePuy; nonconsulting fees from Arthrex; and hospitality payments from the Musculoskeletal Transplant Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Aboalata M, Plath JE, Seppel G, Juretzko J, Vogt S, Imhoff AB. Results of arthroscopic Bankart repair for anterior-inferior shoulder instability at 13-year follow-up. Am J Sports Med. 2016;45(4):782–787. - PubMed
-
- Alberta FG, ElAttrache NS, Bissell S, et al. The development and validation of a functional assessment tool for the upper extremity in the overhead athlete. Am J Sports Med. 2010;38(5):903–911. - PubMed
-
- Anthony CA, Glass NA, Hancock K, Bollier M, Wolf BR, Hettrich CM. Performance of PROMIS instruments in patients with shoulder instability. Am J Sports Med. 2016;45(2):449–453. - PubMed
-
- Cleveland Clinic OME Group, Piuzzi NS, Strnad G, et al. Implementing a scientifically valid, cost-effective, and scalable data collection system at point of care: the Cleveland Clinic OME cohort. J Bone Joint Surg Am. 2019;101(5):458–464. - PubMed
-
- Hawkins RJ, Thigpen CA. Selection, implementation, and interpretation of patient-centered shoulder and elbow outcomes. J Shoulder Elbow Surg. 2018;27(2):357–362. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
